




Torpedo Maculopathy

 Save as PDF
Save as PDFABSTRACT
BACKGROUND
Torpedo maculopathy is a rare condition resulting in malformation of the outer retina. These lesions are often asymptomatic and found incidentally during routine eye examination. Although typically benign, there are rare reports of associated complications requiring treatment. Appropriate monitoring is thus required.
CASE REPORT
A 47-year-old Native American female presented as a new patient seeking to establish routine care. She reports being told of a “birthmark” in the right eye at her first eye exam 20 years ago, and that this birthmark had not caused any changesto her vision. She denied changes in vision and any symptoms associated with said birthmark. She had not had another eye exam within the past 20 years.
CONCLUSION
Torpedo maculopathy is a rare retinal lesion that typically has no visual significance. However, the ability to correctly identify and differentiate this lesion from other macular pathology remains critical. Observation without intervention is appropriate for most cases, but a timely referral should be made in cases where neovascularization is suspected.
Keywords: torpedo maculopathy, retina, macula, optical coherence tomography
INTRODUCTION
Torpedo maculopathy (TM) is a rare, congenital lesion of the retinal pigmented epithelium (RPE). Incidences are thought to be about 2 in 100,000 people, although this figure may be misleadingly low given these lesions are often asymptomatic and discovered during routine care.1 Torpedo maculopathy lesions are typically unilateral, “torpedo” shaped lesions with a pointed tip towards the macula. They tend to be located just temporal to the fovea, but inferior variants have been reported as well.2 These lesions are typically thought to be stationary, although there are case reports of the development of associated macular neovascularization.3 This case report will discuss the etiology, management, and additional ancillary testing measures of torpedo maculopathy.
CASE REPORT
A 47-year-old Native American female presented as a new patient seeking to establish routine care. She reported gradual worsening of her near vision but managed this well with over-the-counter reading glasses. Otherwise, she had no complaints, concerns, or changes in vision. She reports a 20-year history of a “birthmark” in the right eye discovered at her first eye exam. To her knowledge, the birthmark had not caused any changes or had visual significance. To her recollection, observation was recommended at the first and only eye exam. Her medical history was remarkable for hypertension, which was well controlled on two oral medications. Her family ocular and medical history are unremarkable.
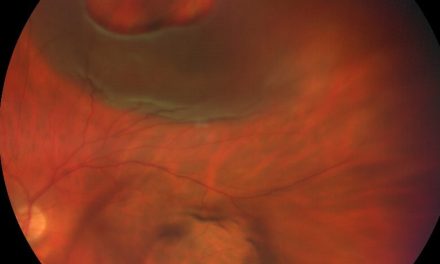
Uncorrected visual acuity was 20/20 at distance OD/OS, near vision was also 20/20 OD/OS with age appropriate near correction. Entrance testing and anterior segment examination were unremarkable; intraocular pressure was 20 mmHg OD and OS via Goldmann applanation tonometry. Dilated fundus examination of the right eye revealed a ~ 0.5 DD hypopigmented lesion temporal to the macula, with a slightly pointed leading edge proximal to the fovea, and a more rounded edge at the distal aspect of the lesion (Figure 1). There was no evidence of fluid or hemorrhage adjacent to the lesion, and there were no other pertinent findings in the right eye. The left eye fundus exam was unremarkable.

Figure 1. Fundus photo of the right eye showing a hypopigmented lesion at the temporal macula.
OCT imaging revealed attenuation of both the ellipsoid and interdigitation zone (Figure 2). The underlying Bruch’s membrane was flat without breaks. The choroid appeared grossly intact, and the foveal ellipsoid zone was spared. There was no evidence of either subretinal or intraretinal fluid.

Figure 2. OCT imaging showing attenuation of both the ellipsoid and interdigitation zone.
Given the long history and characteristic findings of the lesion, a diagnosis of torpedo maculopathy was made. Observation was recommended. The patient requested to only be examined once yearly, but agreed to use an Amsler grid in the meantime and return sooner if any changes were noted.
DISCUSSION
First described by Roseman and Gass in 1992 as a “hypopigmented nevus of the retinal pigmented epithelium,” torpedo maculopathy is a stationary, congenital lesion of the outer retina that results in disruption of the RPE and photoreceptors.4 There is a scarcity of literature on the topic, and pathophysiology is poorly understood. Although typically thought to be a benign lesion, there are a small number of case reports describing associated macular neovascularization, including in pediatric patients.1,5
The exact etiology is unknown; however, one popular theory speculates that this condition is due to an embryological defect in the fetal temporal bulge. Essentially, the fetal temporal bulge is a dense cluster of RPE cells present in the developing retina that is most prominent around 4-6 months of gestation that gradually dissipates leading up to birth. It is thought that this cluster of cells goes on to spread out as the retina develops, and eventually makes up the flat RPE layer we routinely see in patients. This bulge is present temporally to the macula, in the same area where TM lesions go on to develop. Given the uniformity of shape and location of these lesions and their known congenital nature/correspondence with a developmental landmark, it is thought that a persistent defect in the fetal temporal bulge may lead to these characteristic lesions.6 Other proposed theories include fetal chorioretinitis and anomalous choroidal vasculature development.
Increased access to OCT imaging has allowed for these lesions to be further quantified into type 1 or type 2 lesions. In both types, there is attenuation of the ellipsoid zone and interdigitation zone. Type 2 lesions are defined by also having outer retinal cavitations, whereas type 1 lesions do not display this finding. Excavation may or may not be present in both lesion types.7 Microperimetry testing often displays a dense scotoma associated with both lesion types. Our patient’s lesion would be classified as type 1 given the lack of cavitation.
Observation without intervention is typically appropriate for most cases. Although these lesions are stationary, continued observation remains important given the rare chance of macular neovascularization (MNV). There is almost no literature management recommendations for TM associated MNV, although the few cases reported indicate that these lesions are responsive to treatment with intravitreal injection of anti-vascular endothelial growth factor therapy.1
The differential diagnosis is somewhat broad; a non-exhaustive list may include congenital hypertrophy of the RPE, a variety of macular dystrophies, macular degeneration, sequelae of central serous chorioretinopathy, hydroxychloroquine toxicity, and various neoplastic disorders. The characteristic shape, coloration, and location of TM lesions are likely the most helpful diagnostic factors. The congenital nature is also helpful if identified early in life, as this can suggest against processes associated with aging. Of course, it is possible for a patient to present with both TM and one or more of the conditions listed above. If the diagnosis is unclear or multiple diagnoses are being considered, more frequent observation and/or referral may be advisable. It is imperative to not misdiagnose a progressive condition such as macular degeneration or hydroxychloroquine toxicity as TM, as the consequences of mismanagement of these conditions can be devastating.
CONCLUSION
Torpedo maculopathy is a rare, congenital lesion of the retinal pigmented epithelium. Typically benign, these unique lesions are often best managed with observation. While these lesions carry a low risk for macular neovascularization, they must be routinely observed due to this risk. Appropriate treatment or referral to an appropriate specialist should be made in cases of macular neovascularization. There is a need for further research in this topic to better understand the pathophysiology and epidemiology of this condition.
REFERENCES
- Shirley K, O’Neill M, Gamble R, Ramsey A, McLoone E. Torpedo maculopathy: disease spectrum and associated choroidal neovascularisation in a paediatric population. Eye (Lond). 2018 Aug;32(8):1315-1320. doi: 10.1038/s41433-018-0074-7. Epub 2018 Mar 20. PMID: 29556011; PMCID: PMC6085330.
- Smith MJ, Sia DIT, Greve M. Torpedo maculopathy-inferior variant. Can J Ophthalmol. 2021 Mar 18:S0008-4182(21)00045-4. doi: 10.1016/j.jcjo.2021.02.008. Epub ahead of print. PMID: 33745872.
- Jurjevic D, Böni C, Barthelmes D, Fasler K, Becker M, Michels S, et al. Torpedo Maculopathy Associated with Choroidal Neovascularization. Klin Monbl Augenheilkd. 2017 Apr;234(4):508-514. English. doi: 10.1055/s-0043-100230. Epub 2017 May 3. PMID: 28470647.
- Roseman RL, Gass JD. Solitary hypopigmented nevus of the retinal pigment epithelium in the macula. Arch Ophthalmol. 1992 Oct;110(10):1358-9. doi: 10.1001/archopht.1992.01080220020005. Erratum in: Arch Ophthalmol 1992 Dec;110(12):1762. PMID: 1417528.
- Parodi MB, Romano F, Montagna M, Albertini GC, Pierro L, Arrigo A, et al. Choroidal Neovascularization in Torpedo Maculopathy Assessed on Optical Coherence Tomography Angiography. Ophthalmic Surg Lasers Imaging Retina. 2018 Nov 1;49(11):e210-e213. doi: 10.3928/23258160-20181101-20. PMID: 30457658.
- Shields CL, Guzman JM, Shapiro MJ, Fogel LE, Shields JA. Torpedo Maculopathy at the Site of the Fetal “Bulge”. Arch Ophthalmol. 2010;128(4):499–501. doi:10.1001/archophthalmol.2010.29
- Wong EN, Fraser-Bell S, Hunyor AP, Chen FK. Novel optical coherence tomography classification of torpedo maculopathy. Clin Exp Ophthalmol. 2015 May-Jun;43(4):342-8. doi: 10.1111/ceo.12435. Epub 2014 Nov 7. PMID: 25266677.

Dr. Provost graduated from New England College of Optometry in 2022 and then completed an ocular disease residency at VA Boston Jamaica Plain from 2022-2023. He is currently an Assistant Professor of Optometry at Northeastern State University Oklahoma College of Optometry, and an attending optometrist at the W.W. Hastings Hospital in Tahlequah, Oklahoma.



{kind=link}