



Lymphoma Masquerading as a Hordeolum

 Save as PDF
Save as PDFABSTRACT
BACKGROUND
Sinonasal B-cell lymphomas are rare extranodal malignancies that frequently present with orbital manifestations mimicking benign eyelid conditions. These aggressive tumors may cause diagnostic delays, and systemic metastases can be present even when symptoms appear localized to the eye.
CASE REPORT
A 68-year-old white male with cognitive impairment secondary to prior cerebrovascular accident presented with left upper eyelid swelling initially diagnosed as hordeolum with conjunctivitis. Despite topical ofloxacin therapy, the condition rapidly progressed over 48 hours to involve the entire upper and lower eyelids. Oral amoxicillin-clavulanate was initiated for suspected preseptal cellulitis, but the patient subsequently developed restricted adduction and intermittent diplopia, prompting urgent imaging. Computed tomography revealed a hypodense mass in the left ethmoid sinus with lamina papyracea destruction, orbital invasion, and mass effect on the medial rectus muscle. Biopsy confirmed B-cell lymphoma. Surgical drainage provided temporary relief, but staging revealed extensive osseous and visceral metastases consistent with Stage 4 non-Hodgkin lymphoma. Following minimal response to chemotherapy and progressive pain, the patient transitioned to hospice care and died approximately two months after initial presentation.
CONCLUSION
This case illustrates the critical importance of recognizing serious features in patients presenting with eyelid swelling, particularly rapid progression despite appropriate antimicrobial therapy and development of extraocular motility restrictions. Sinonasal lymphomas can breach the lamina papyracea and invade orbital structures while clinically masquerading as hordeolum or preseptal cellulitis. The presence of systemic metastases at diagnosis, despite apparently localized ocular symptoms, underscores the aggressive nature of Stage 4 sinonasal lymphomas. Prompt recognition, urgent imaging, and expedited biopsy are essential for diagnosis, though prognosis remains poor in elderly patients with advanced-stage disease and limited treatment tolerance.
Keywords: B-cell lymphoma; non-Hodgkin lymphoma; ethmoid sinus; hordeolum; preseptal cellulitis; orbital cellulitis; bone metastases, CT-Scan
INTRODUCTION
Primary sinonasal lymphomas constitute a rare subset of extranodal non-Hodgkin lymphomas (NHL), representing approximately 0.61% of all non-Hodgkin lymphomas annually, with an estimated incidence of 0.14 per 100,000 person-years.1 Within this category, diffuse large B-cell lymphoma (DLBCL) predominates, accounting for over 80% of primary sinonasal B-cell lymphomas. These aggressive malignancies most commonly arise in the maxillary sinus, followed by the nasal cavity and ethmoid sinus, with frequent extension to adjacent structures, including the orbit.2
The anatomic proximity of the ethmoid sinus to the orbit, separated only by the thin lamina papyracea, provides a pathway for direct tumor extension into orbital structures.3 Studies indicate that approximately 38% of ethmoid sinus lymphomas demonstrate orbital extension at presentation, often manifesting as proptosis, diplopia, ophthalmoplegia, or periorbital swelling.1 This orbital involvement creates substantial diagnostic challenges, as the clinical presentation may closely mimic more common and benign conditions such as a hordeolum, preseptal cellulitis, or orbital cellulitis.4
The following is a case of primary ethmoid sinus DLBCL with orbital invasion that initially masqueraded as a hordeolum and preseptal cellulitis, ultimately diagnosed as stage 4 non-Hodgkin lymphoma with extensive osseous and visceral metastases. This case highlights critical clinical decision points, red flags requiring urgent clinical management, and the aggressive nature of advanced stage sinonasal lymphoma in elderly patients.
CASE REPORT
A 68-year-old white male was referred from an urgent care clinic to the eye clinic for left upper eyelid swelling that blocked his vision nasally. He had a history of a cerebrovascular accident that led to impaired cognition and slow response, so his elder sister accompanied him and served as his primary historian. His last comprehensive eye exam a few months earlier was unremarkable. His medical history included benign prostatic hyperplasia, diabetes, and hyperlipidemia, for which he took amlodipine, aspirin, atorvastatin, lisinopril, and metformin.
Urgent care diagnosed the condition as a hordeolum with associated conjunctivitis, and he was prescribed topical ofloxacin four times a day in his left eye. Additionally, the urgent care provider instructed the patient to present to the eye clinic that same day for further evaluation.
At the initial visit, uncorrected visual acuity was 20/50 OD and 20/150 OS. The patient did not like to wear glasses and was not able to be refracted or pin-holed. Extraocular muscle motility was full without restrictions, pain, or diplopia; confrontation fields were full OD and OS, but somewhat restricted superior-nasally OS; and pupils were equal, round, and reactive to light with no afferent pupillary defect. Anterior segment findings were remarkable for a large area of eyelid edema of the nasal upper lid with trace surrounding erythema and mild mucous discharge. Intraocular pressures were 14 mmHg in each eye via Goldmann applanation tonometry. He was advised to continue the ofloxacin, start erythromycin ointment nightly before bedtime, and use warm compresses. He was scheduled to return to the clinic in one week for follow-up or sooner as needed.
The next day, despite topical antibiotic treatment, the patient returned because the left eyelid swelling had worsened, spreading temporally across the upper lid and lower lid (Figure 1). Visual acuity was stable; there was no fever, no diplopia, and no pain with eye movement. Preseptal cellulitis was suspected, and he was prescribed oral Augmentin 875/125 mg bid for ten days and instructed to continue warm compresses twice daily. He was scheduled to return the following afternoon for closer monitoring.
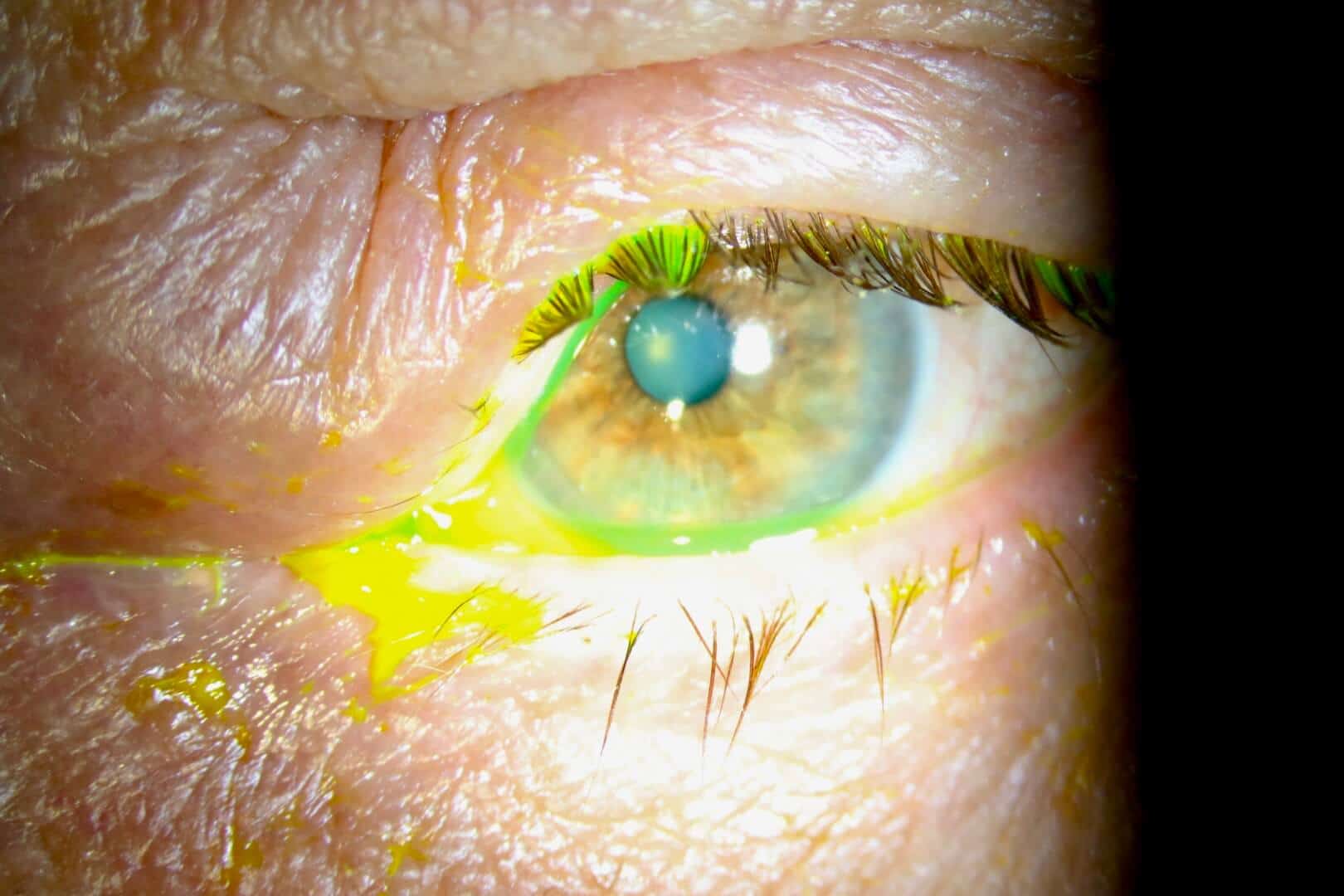
Figure 1. Anterior segment photo of left eye on day 2 with diffuse upper eyelid swelling nasally.
After taking a few tablets of Augmentin, the lid swelling worsened further, so his sister brought him back to the clinic early the next morning. Although his vision was stable, he had restricted adduction OS and intermittent diplopia (Figure 2). Orbital cellulitis was highly likely, so he was sent for an urgent computed tomography (CT) scan without contrast of the orbit. Contrast was withheld, as the patient was on metformin. The CT scans showed a hypodense lesion occupying the left ethmoid sinus, expanding past the lamina papyracea, and exerting mass effect on the left medial rectus as well as the globe, causing restricted adduction and proptosis (Figures 3 and 4).

Figure 2. Anterior segment photo of left eye on day 3 with significant upper and lower lid edema.

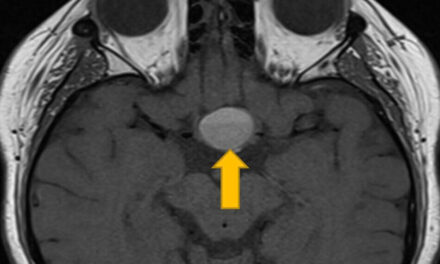
Figure 3. A representative axial CT scan of the orbit without contrast (soft tissue window) on day 3 showing a large hypodense lesion (arrow) in the left ethmoid sinus.

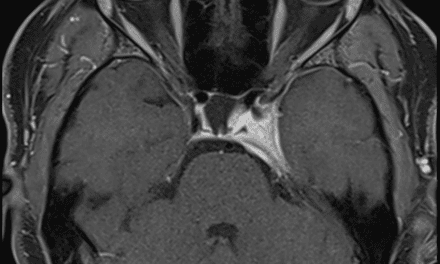
Figure 4. A representative coronal CT scan of the orbit without contrast (soft tissue window) on day 3 showing a large lesion (arrow) in the left ethmoid sinus.
The patient was sent to the emergency department at a small local hospital and subsequently medically evacuated to a larger medical center a few hours away for further management. An MRI and biopsy of the tissue confirmed the diagnosis of B-cell lymphoma of the left ethmoid sinus that extended into the left orbit and eyelids. A neurosurgeon drained the ethmoid sinus into the maxillary sinus to reduce the edema, and the patient was returned to a local cancer care facility for oncologic management.
Two weeks after the initial visit, the eyelid swelling had significantly reduced but still persisted (Figure 5). His vision was stable without ocular pain, but he developed progressive upper left back and shoulder pain. The PET scan at the cancer center showed extensive metastases to his bones, including the left shoulder region, as well as other organs. Flow cytometry staged the cancer as stage 4 B-cell non-Hodgkin lymphoma. Chemotherapy was attempted twice with minimal improvement. Because of increasing pain and poor response to chemotherapy, the patient and his family decided to discontinue therapy. He was transferred to hospice for pain relief and comfort, and he passed away surrounded by family about two months later.

Figure 5. Anterior segment photo of the left eye on day 15 after drainage of fluid from the ethmoid sinus.
DISCUSSION
Hordeola and chalazia are among the most common eyelid conditions encountered in primary eye care, affecting patients of all ages. The typical presentation includes localized eyelid swelling with erythema, tenderness, and sometimes a visible pustule. Conservative management with warm compresses typically results in spontaneous drainage and resolution within days to weeks, and topical antibiotics may be prescribed to treat associated conjunctivitis or blepharitis and expedite recovery. When this treatment fails or symptoms worsen, a broader differential diagnosis becomes necessary.
In this case, the rapid exacerbation of signs and symptoms despite initial topical antibiotics use suggested a more serious condition of preseptal cellulitis; hence, oral antibiotics were prescribed.5 The worsening of swelling and restriction of extraocular motility despite oral antibiotics indicated that local infection might not be the primary etiology. Therefore, urgent re-evaluation with orbital imaging was needed to rule out orbital cellulitis or other space-occupying lesions. The differential diagnosis for periorbital swelling with restricted motility includes orbital cellulitis with subperiosteal abscess, invasive fungal infection (particularly in those who are immunocompromised), cavernous sinus thrombosis, thyroid eye disease, idiopathic orbital inflammatory syndrome (orbital pseudotumor), and orbital mass lesions, including primary tumors or metastases.6
NHLs are a heterogeneous group of malignant lymphoid neoplasms that typically arise in lymph nodes but may also present primarily in extranodal organs such as the gastrointestinal tract, skin, or central nervous system. Nodal NHL is confined to lymphoid tissues (lymph nodes, spleen, thymus), whereas extranodal disease originates in, or is predominantly localized to, non-lymphatic sites, with up to one‑third of NHLs arising outside lymph nodes. In the Lugano/Ann Arbor system, stage 1 involves a single nodal region or single extralymphatic organ; stage 2 involves two or more nodal regions on the same side of the diaphragm, with or without limited contiguous extranodal extension. Stage 3 is characterized by nodal involvement on both sides of the diaphragm, sometimes with spleen or contiguous extranodal involvement. Stage 4 NHL, characterized by disseminated disease involving multiple extranodal sites or bone marrow, presents additional therapeutic challenges. While overall 5-year survival rates for stage 4 NHL range from 55% to 64% across all subtypes, elderly patients with comorbidities, cognitive impairment, and poor performance status experience substantially worse outcomes.7,8 Treatment typically involves combination chemoimmunotherapy with rituximab plus cyclophosphamide, doxorubicin (hydroxydaunorubicin), vincristine (Oncovin), and prednisone (R-CHOP), though only 46% of elderly patients receive standard-dose therapy because of concerns regarding treatment tolerance and toxicity.9
NHL can involve virtually every compartment of the eye and orbit, including the eyelids, conjunctiva, lacrimal gland and sac, extraocular muscles, orbital fat, uvea, retina, vitreous, and optic nerve sheath. Ocular adnexal lymphomas (OALs) account for about 1–2% of all non-Hodgkin lymphomas and 5–15% of extranodal lymphomas, yet they are the most common primary orbital malignancy in adults. Within the ocular adnexa, the orbit and conjunctiva are typically the most frequently affected sites (each around 25–40%), as in this case, followed by the lacrimal gland and eyelid, whereas lacrimal drainage system involvement is distinctly uncommon.10,11 Bone involvement occurs in approximately 16% of patients with DLBCL at diagnosis and can manifest pain, pathological fractures, or incidental findings on imaging.12 Contrary to historical perceptions, osseous involvement in DLBCL does not independently portend worse prognosis when appropriately treated, with 5-year progression-free survival of 66% in advanced-stage disease with bone involvement, like nodal disease.1 However, the presence of stage 4 disease with multiple metastatic sites indicates aggressive biology and warrants multidisciplinary management.
Among elderly patients who receive standard chemotherapy, treatment-related toxicity is substantial. Grade 3 or 4 adverse events occur in 65% to 67% of cases, and only 56% complete six or more cycles of treatment.13 In patients aged 75 years and older with DLBCL, cause-specific survival at three years is approximately 58%, with overall survival of 51%. Pre-existing cognitive impairment, as in this patient, further complicates treatment. Cognitive impairment, present in approximately 20% to 30% of elderly cancer patients at baseline, is associated with difficulty processing medical information, providing informed consent, adhering to complex treatment regimens, and experiencing a higher risk of chemotherapy-related toxicity and further cognitive decline.14,15
In this case, the patient’s minimal response to two cycles of chemotherapy, combined with significant treatment-related toxicity and progressive bone pain, led to the patient and family’s decision to discontinue curative-intent therapy and transition to hospice care. This trajectory is unfortunately common in elderly patients with stage 4 sinonasal lymphoma and poor prognostic features. The patient’s transition to hospice care approximately six weeks after diagnosis, though relatively rapid, was appropriate given his minimal response to chemotherapy, significant treatment-related toxicity, progressive bone pain, declining functional status, and overall clinical trajectory. Hospice optimized his pain management and provided comfort-focused care in his final weeks, allowing him to die peacefully with his family at his bedside.
CONCLUSION
This case of ethmoid sinus diffuse large B-cell lymphoma with orbital invasion and stage 4 systemic metastases illustrates the critical importance of clinical vigilance when evaluating eyelid swelling. What initially appeared to be a simple hordeolum progressed rapidly, despite appropriate antimicrobial therapy, ultimately revealing aggressive sinonasal malignancy with extensive systemic disease. Sinonasal lymphomas, though rare, can masquerade as benign eyelid conditions such as hordeolum or preseptal cellulitis. Optometrists must maintain high suspicion for malignancy when eyelid swelling fails to respond to appropriate therapy and progresses rapidly. Prompt recognition of serious clinical features and co-management with other specialists for expedited imaging and definitive diagnosis are essential to optimize outcomes and quality of life for patients with these aggressive malignancies.
REFERENCES
- Havelund BM, Mikic S, Diaz A, Schwartz K, Schreiber D, Grunwald MR, et al. Sinonasal B-cell lymphomas: A nationwide cohort study, with an emphasis on treatment and prognostic factors. Head Neck. 2022;44:1101-16.
- Pfreundschuh M, Trümper L, Österborg A, Pettengell R, Trneny M, Imrie K, et al. CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: a randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol. 2006;7:379-91.
- Olsen TG, Heegaard S. Orbital lymphoma. Surv Ophthalmol. 2019;64:45-66.
- Givner LB. Periorbital versus orbital cellulitis. Pediatr Infect Dis J. 2002;21:1157-8.
- Hauser A, Fogarasi S. Periorbital and orbital cellulitis. Pediatr Rev. 2010;31:242-9.
- Boltezar L, Strbac D, Pizem J, Hawlina G. Ocular adnexal lymphoma: a retrospective study and review of the literature. Radiol Oncol. 2024;58:416-24.
- City of Hope. Non-Hodgkin lymphoma stages. [Internet]. 2022 Aug [Cited 2026 Mar 18]. Available from: https://www.cancercenter.com/cancer-types/non-hodgkin-lymphoma/stages
- Nabhan C, Byrtek M, Rai A, Dawson K, Zhou X, Link BK, et al. Diffuse large B-cell lymphoma in adults aged 75 years and older: patterns of care and survival in the United States. Cancer. 2013;119:2700-8.
- Cure Today. Stage 4 Lymphoma [Internet]. 2022 May [cited 2026 Jan 30]. Available from: https://www.curetoday.com/view/stage-4-lymphoma
- Hatef E, Roberts D, Malaughlin P, et al. Prevalence and Nature of Systemic Involvement and Stage at Initial Examination in Patients With Orbital and Ocular Adnexal Lymphoma. Arch Ophthal. 2007;125;(12):1663-1667.
- Amir A, Amir B, Sheikh S. Primary ocular adnexal mantle cell lymphoma with distant spread and involvement of the contralateral eye one year later; a case report and literature review. Journal of Surgical Case Reports, Volume 2024, Issue 6, https://doi.org/10.1093/jscr/rjae414
- Choi J, Raghavan V, Fox E, Sehn LH, Scott DW, Connors JM, et al. Primary bone diffuse large B-cell lymphoma: a unique clinical entity with favorable outcome. Haematologica. 2023;108:3210-9.
- Schöder H, Moskowitz AJ, Gönen M, Batlevi CL, Cadzin BR, Hamlin PA, et al. Diffuse large B-cell lymphoma involving osseous sites: response assessment by positron emission tomography. Haematologica. 2024;109:424-33.
- Mohile SG, Dale W, Somerfield MR, Schonberg MA, Boyd CM, Burhenn PS, et al. Practical assessment and management of vulnerabilities in older patients receiving chemotherapy: ASCO Guideline for Geriatric Oncology. J Clin Oncol. 2018;36:2326-47.
- Odejide OO, Salas Coronado DY, Watts CD, Wright AA, Abel GA. End-of-life care for blood cancers: a series of focus groups with hematologic oncologists. J Oncol Pract. 2014;10:e396-403.

Len Koh is a staff optometrist and residency site director at the Mann-Grandstaff VA Medical Center in Spokane, Washington. He is grateful for the opportunity to train students and residents while providing high-quality eye care to veterans. Outside of work, he and his wife enjoy raising their two teenagers and spending time together in the outdoors.

Graduated from Pacific University in 2025 and completing residency at the Spokane VA Medical Center Eye Clinic 2026.
Dr. Bice graduated from Pacific University College of Optometry in 2020 and completed her residency in ocular disease at the Mann-Grandstaff VAMC in 2021. She returned to Mann-Grandstaff VAMC in 2024 and is now the co-director of student program.
Mann-Grandstaff VA Medical Center Chief of Optometry Services

{kind=link}