



Visual and Quality-of-Life Effects of Aponeurotic Ptosis in Older Adults

 Save as PDF
Save as PDFABSTRACT
Significance:
Bilateral aponeurotic ptosis in older adults significantly reduces vision-related quality of life, especially for near visual activities and mental well-being.
Purpose:
To assess the effect of bilateral aponeurotic ptosis on visual acuity and vision-related quality of life in older adults.
Methods:
A cross-sectional, observational, and analytical study was conducted at a tertiary ophthalmology referral center in Mexico City. Fifty patients aged 60–80 years with bilateral aponeurotic ptosis were consecutively recruited between October 2024 and April 2025. Visual acuity was measured using the Snellen chart, and quality of life was assessed with the National Eye Institute Visual Function Questionnaire (NEI VFQ-25). Associations were analyzed using multiple linear regression adjusted for age and sex.
Results:
The mean age of participants was 72 years, and 52% were female. The mean best-corrected visual acuity was 20/30 in the better eye. The mean NEI VFQ-25 score was 61.3 (SD 5.2). No significant sex differences were observed (p = 0.42). The lowest-scoring domains were near activities, role difficulties, and mental health.
Conclusions:
Aponeurotic palpebral ptosis negatively affects both visual function and vision-related quality of life in older adults, particularly in tasks requiring near vision and in mental well-being. These findings highlight the need for a comprehensive and patient-centered approach that addresses both the functional and psychological aspects of this condition.
Keywords: Ptosis; Eyelid Diseases; Visual Acuity; Quality of Life; Aged; Cross-Sectional Studies
introduction
Aponeurotic blepharoptosis, or involutional ptosis, is the most prevalent form of upper eyelid drooping in the geriatric population.1 Its etiology is primarily degenerative, characterized by the gradual dehiscence, disinsertion, or attenuation of the levator palpebrae superioris aponeurosis.2 This process is often exacerbated by chronic inflammation, intraocular surgery, or repetitive eyelid manipulation, leading to a functional deficit in vertical palpebral fissure displacement despite normal levator muscle function.
While frequently dismissed as a natural consequence of aging or a purely aesthetic concern, the impact of aponeurotic ptosis can be profound. Beyond the mechanical obstruction of the superior visual field, patients often compensate through chronic contraction of the frontalis muscle, resulting in persistent cephalalgia and physical fatigue. Current treatment is predominantly surgical, involving the advancement or repair of the aponeurosis to restore the lid margin to its physiological position. These surgical interventions have demonstrated significant benefits, substantially improving visual functionality and, consequently, the patient’s overall quality of life.3 However, clinical success is traditionally measured by anatomical height rather than the patient’s perceived functional recovery.
The global literature underscores the magnitude of this condition. Sridharan et al. (1995) reported a prevalence of 11.5% in patients over 50 years in the UK,4 while more recent studies in Asian populations, such as that by Hu et al. (2024), show rates as high as 32.8% in those over 70.5 In the Americas, Matossian et al. (2024) recently reported that 73.4% of patients aged 50 and older in a United States population had blepharoptosis in at least one eye.6
In Mexico, data from a leading tertiary care ophthalmology center revealed that between 2023 and 2024 alone, 2,547 cases were documented, emphasizing a significant but under-studied public health burden in the region. Despite these clinical records, the specific prevalence of ptosis in the Mexican geriatric population has not been directly investigated. Data from international cohorts cannot be directly extrapolated to Mexico due to differences in demographics and healthcare access; therefore, in the absence of local epidemiological studies, providing a precise prevalence rate for this demographic remains a challenge.
Despite these figures, a substantial knowledge gap remains regarding how the severity of bilateral ptosis correlates with visual acuity, and clinical metrics alone do not fully capture the patient’s lived experience.7 According to the World Health Organization (WHO), quality of life (QoL) is a broad concept defined as a person’s perception of their position in life within their cultural context, influenced by physical health, psychological state, and social relationships.8 The National Eye Institute Visual Function Questionnaire (NEI VFQ-25) scale is utilized to evaluate vision-specific health dimensions. This instrument transforms scores into a 0–100 scale, where higher scores indicate better function across subscales such as mental health, social functioning, and dependency.9 The scale is widely validated in the United States, where multiple studies have demonstrated its reliability and validity across various ocular conditions; for instance, Sivaprasad et al. confirmed its effectiveness as a tool for patients with geographic atrophy, highlighting its ability to capture the functional impact of progressive visual loss.10 While validated in the United States and used in studies like “Proyecto VER” for Hispanic populations,11 there is a scarcity of studies dedicated exclusively to the geriatric sector in Mexico.
By integrating standardized visual examinations with the NEI VFQ-25, this study aims to fill this critical void. The purpose of this study is to evaluate the impact of bilateral aponeurotic ptosis on visual acuity and vision-related quality of life in older adults at a tertiary referral hospital. We hypothesize that increased ptosis severity is associated with a measurable decrease in visual acuity and a significant decline in specific QoL domains, particularly mental health and near-vision activities, providing a baseline for a more patient-centered approach to surgical indication.
methods
Study Design and Population:
This cross-sectional, observational, and analytical study was conducted at a tertiary ophthalmology referral center in Mexico City between October 2024 and April 2025. Adults aged 60–80 years diagnosed with bilateral aponeurotic palpebral ptosis were included. Inclusion criteria were mild to moderate dry eye under treatment, prior uncomplicated cataract surgery, and best-corrected visual acuity of approximately 20/40 or better using corrective lenses. Exclusion criteria included unilateral ptosis, eyelid masses, glaucoma, cataracts, and systemic conditions that could affect visual function, such as poorly controlled diabetes mellitus (including diabetic retinopathy or diabetic optic neuropathy) and systemic hypertension with ocular involvement (e.g., hypertensive retinopathy or hypertensive optic neuropathy).
Variable Identification:
To ensure clarity in the analytical model, variables were explicitly categorized as follows:
- Independent Variables: The primary independent variable was the degree of ptosis, measured in millimeters of upper eyelid drooping [Margin-Reflex Distance 1 (MRD-1)]. This was analyzed both as a continuous variable (mm) and categorized (mild: 2–3 mm, moderate: 1 mm, severe: ≤0 mm).
- Dependent Variables: Two primary outcomes were measured: (1) Visual Acuity (VA), recorded as a Snellen fraction and converted to LogMAR for statistical analysis; and (2) Vision-Related Quality of Life, determined by the composite and subscale scores of the NEI VFQ-25. Items within each domain are converted to a score ranging from 0 to 100 (maximum score), and the overall composite is calculated by averaging these results. A higher value indicates better vision-specific quality of life.
- Potential Confounders and Covariates: Age and sex were identified as primary confounders. While data on race were not collected as the study population was a relatively homogeneous Mexican mestizo cohort, prior ocular surgery (specifically uncomplicated cataract surgery) and comorbidities (controlled diabetes and hypertension) were recorded and considered as potential factors influencing baseline visual function.
Procedures and Data Collection:
The degree of ptosis was determined by measuring MRD-1 following standard clinical examination procedures. Visual acuity was assessed using the Snellen chart, and quality of life was evaluated using the validated NEI VFQ-25. Additionally, two ad hoc questions were specifically integrated into the assessment to evaluate postural pain associated with compensatory head positioning, as the original questionnaire does not explicitly address physical discomfort related to ptosis. These supplemental questions assessed the presence and intensity of pain, categorized as none, mild, moderate, or very severe. All evaluations were performed by trained medical personnel to minimize measurement bias.
Statistical Analysis:
Quantitative variables were summarized with means and standard deviations. The core of our analysis used Multiple Linear Regression models to measure two specific associations:
- The association between the severity of ptosis (MRD-1) and visual acuity.
- The association between the severity of ptosis (MRD-1) and vision-related quality of life (NEI VFQ-25 scores).
These models were adjusted for age and sex as covariates to control for their potential confounding effects on the relationship between physical eyelid position and perceived quality of life. Statistical analyses were performed using IBM SPSS Statistics version 29, with a significance level of p < 0.05.
Ethical Considerations:
The study adhered to the Declaration of Helsinki. All participants provided written informed consent, and the protocol was approved by the tertiary referral hospital in México City.
Results
Fifty eligible patients were enrolled, all meeting the inclusion criteria and completing the study. The mean age was 72.1 years (range 60–80). Of the total, 52% (n = 26) were women and 48% (n = 24) were men. Seventy-six percent (n = 38) had systemic comorbidities, primarily systemic arterial hypertension and type 2 diabetes mellitus. None had prior surgical treatment for ptosis. Detailed cohort demographics and clinical characteristics, categorized by ptosis severity, are presented in Table 1.
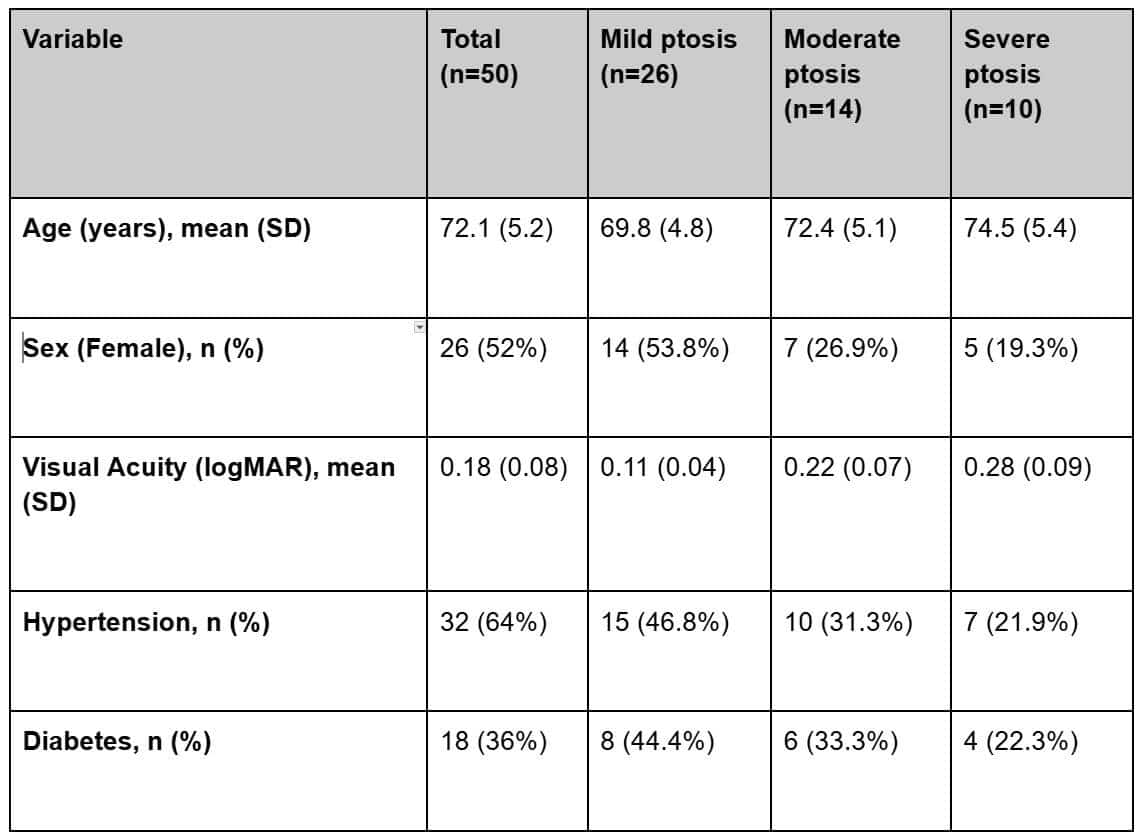
Table 1. Demographics and baseline clinical characteristics of 50 individuals with bilateral aponeurotic ptosis.
Visual acuity was evaluated using the logMAR scale, with an overall mean of 0.18 (95% CI: 0.15–0.21; approximately 20/30 Snellen). The mean NEI VFQ-25 total score was 61.3 (95% CI: 57.1–65.5). When classified by the impact on daily life, 58% of participants (95% CI: 43.2%–71.8%) showed mild quality-of-life impairment and 42% (95% CI: 28.2%–56.8%) moderate impairment.
Regarding physical discomfort, postural pain associated with compensatory head positioning was reported by 54% of the cohort (n = 27; 95% CI: 39.3%–68.2%). Among those experiencing discomfort, the intensity was categorized as mild in 22% (n = 11; 95% CI: 11.5%–36.0%), moderate in 22% (n = 11; 95% CI: 11.5%–36.0%), and very severe in 10% (n = 5; 95% CI: 3.3%–21.8%) of the total sample. Conversely, 46% of patients (n = 23; 95% CI: 31.8%–60.7%) reported no postural or physical pain related to their condition. Detailed scores for physical discomfort and postural pain according to ptosis severity are shown in Table 2. No significant sex differences were found in NEI VFQ-25 scores (men median: 63.9, 95% CI: 58.1–69.7; women median: 60.2, 95% CI: 54.8–65.6; p = 0.42).
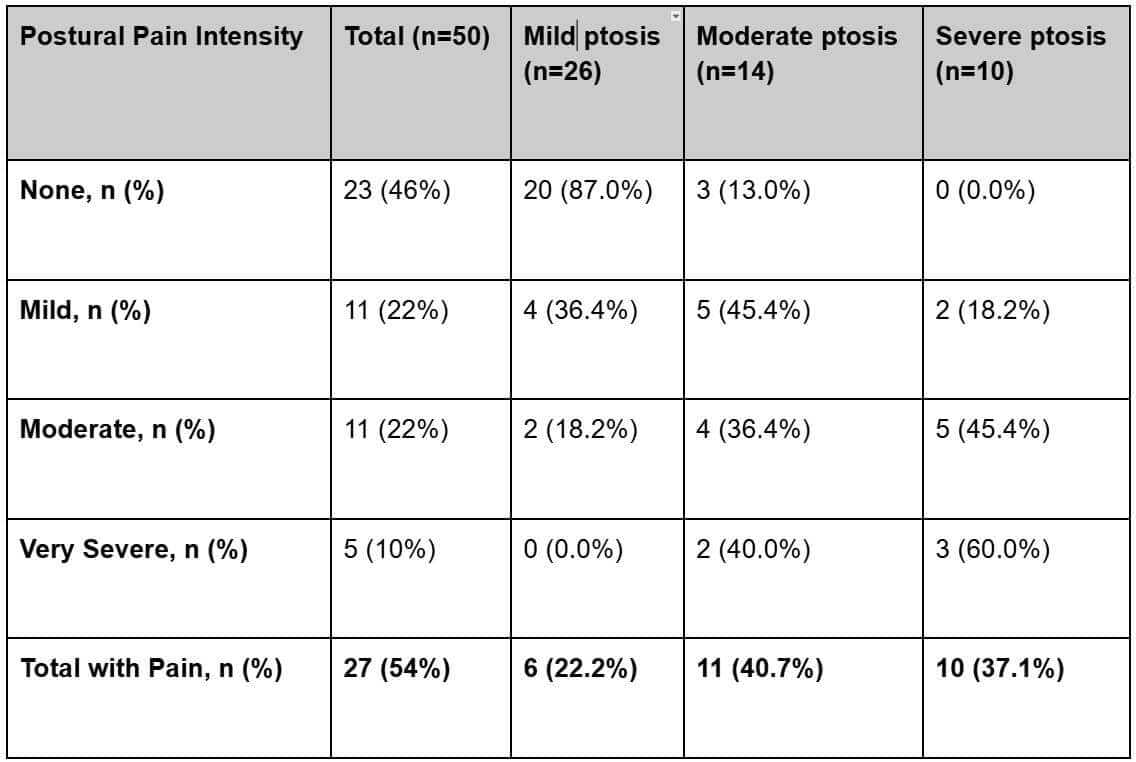
Table 2. Physical discomfort and postural pain scores categorized by ptosis severity.
To evaluate the associations between clinical findings and patient well-being, multivariable linear regression models were used. The analysis confirmed that ptosis severity (MRD-1) was significantly associated with lower quality-of-life scores (beta = -5.12; 95% CI: -6.45 to -3.79; p < 0.001), independently of age and sex. Additionally, visual acuity showed a significant association with the NEI VFQ-25 total score (beta = -3.89; 95% CI: -6.91 to -0.87; p = 0.012). Regression coefficients and 95% confidence intervals are detailed in Table 3. Assumptions for the linear regression models were evaluated through inspection of residual plots, which indicated no major violations of linearity, normality of residuals, or homoscedasticity.
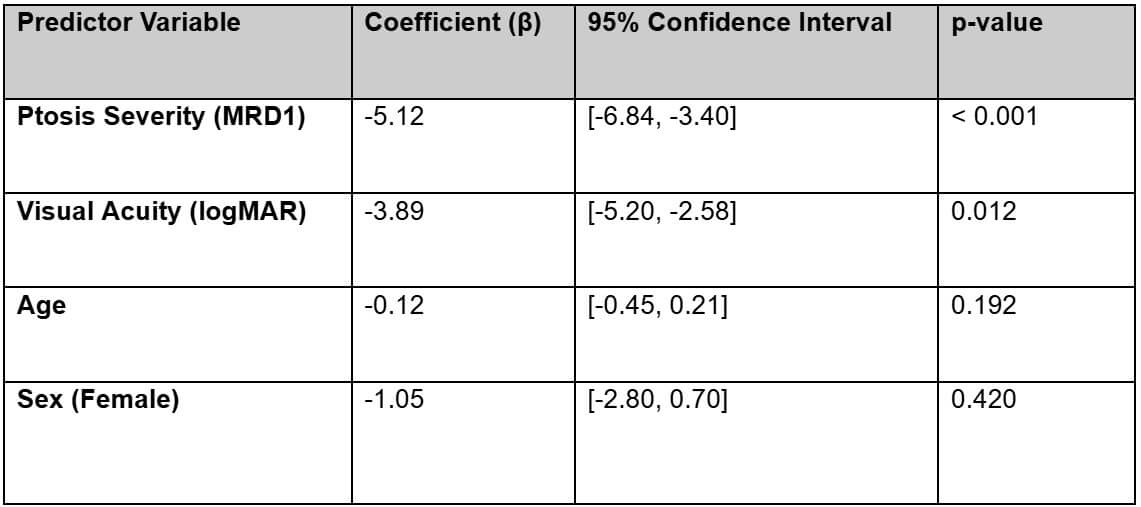
Table 3. Linear regression coefficients and 95% CI examining the association between severity of ptosis and quality of life score on VFQ-25, adjusted for age and sex.
discussion
This study included 50 older adults (mean age 72 years) with bilateral aponeurotic ptosis. The slight majority were women and had systemic comorbidities, primarily hypertension and diabetes. Although many maintained functional visual acuity, most reported some impairment in vision-related quality of life.
Women showed slightly lower NEI VFQ-25 scores, which may reflect greater emotional and aesthetic concern. In the Mexican geriatric population studied, this emotional burden is closely linked to social perception and daily role difficulties, where the patient’s self-image plays a fundamental role in their overall well-being. The severity of ptosis did not always correlate directly with poorer visual acuity or lower NEI VFQ-25 scores, highlighting the relevance of subjective perception.
A key finding is the high prevalence of postural and physical discomfort reported by the participants. This underscores that aponeurotic ptosis imposes a physical strain that goes beyond simple visual obstruction. The chronic effort required to maintain an open palpebral fissure leads to significant physical fatigue. Furthermore, dry eye, even in mild-to-moderate stages, is a relevant factor in exacerbating these symptoms. The interaction between the mechanical eyelid drooping and ocular surface irritation increases the sensation of “heavy eyelids,” directly contributing to lower scores in the “Role Difficulties” and “Mental Health” domains of the quality-of-life assessment.
Limitations include that the planned sample size of 60 participants was not fully achieved, as only 50 patients were ultimately included during the study period due to time constraints and the limited number of eligible cases. The target sample size was estimated using the formula for proportions in a finite population, assuming an 80% confidence level and based on the expected number of eligible patients during the study period. Given the relatively small number of eligible patients available during the study period, recruitment of a larger sample to achieve a higher confidence level was not feasible. Additionally, the NEI VFQ-25 is a self-reported instrument and may therefore be subject to perception bias. Multivariable analyses were limited by the modest sample size. Nevertheless, this study provides valuable insight into the psychosocial and functional impact of ptosis in older adults.
Recognizing both visual and emotional dimensions of ptosis is essential for comprehensive care. Beyond surgical correction, management should address patient self-image, mental health, and daily functioning.
conclusions
Bilateral aponeurotic palpebral ptosis in older adults is associated with reduced vision-related quality of life, particularly in near activities and mental well-being. Although many retain good visual acuity, the functional and psychosocial burden justifies an integrated, patient-centered clinical approach.
references
- Katsuo A, Iwasaki K, Takayanagi R, et al. Evaluation of risk factors for unilateral aponeurotic ptosis using the fellow eye as control: a retrospective study. Clin Ophthalmol. 2024;18:1115–1121.
- Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg. 2003;27(3):193–204.
- Bacharach J, Lee WW, Harrison AR, Freddo TF. A review of acquired blepharoptosis: prevalence, diagnosis, and current treatment options. Eye (Lond). 2021;35(11):2789–2795.
- Sridharan GV, Tallis RC, Leatherbarrow B, Forman WM. A community survey of ptosis of the eyelid and pupil size of elderly people. Age Ageing. 1995;24(1):21–24.
- Hu S, Chen X, Zheng G, Zhao Y, He X, Liu X. The prevalence and risk factors of blepharoptosis in an elderly Asian population. Aesthet Surg J. 2024;43(5):569–579. doi:10.1007/s00266-023-03804-2.
- Matossian C. The prevalence and severity of acquired blepharoptosis in US eye care clinic patients. Clin Ophthalmol. 2024;18:79–83. doi:10.2147/OPTH.S441505.
- García J, Sánchez F, et al. Valoración de la agudeza visual. Rev Esp Salud Pública. 2016;90:e1–e11.
- Instituto Nacional de las Personas Adultas Mayores (INAPAM). Calidad de vida para un envejecimiento saludable. México: INAPAM; 2023.
- Wan Y, Zhao L, Huang C, et al. Validation and comparison of the NEI VFQ-25 and VF-14 in patients with cataracts: a multicenter study. Acta Ophthalmologica. 2021;99(4):e617–e623.
- Sivaprasad S, Tschosik E, Kapre A, et al. Reliability and construct validity of the NEI VFQ-25 in patients with geographic atrophy. Am J Ophthalmol. 2018;190:1–8.
- Broman AT, Munoz B, West SK, et al. Psychometric properties of the NEI-VFQ in a Hispanic population: Proyecto VER. Invest Ophthalmol Vis Sci. 2001;42(3):606–613.

General Practitioner from Mérida, Yucatán, and a proud graduate of UPAEP.



{kind=link}