




Diplopia Detective

 Save as PDF
Save as PDF
Welcome to the Journal of Medical Optometry’s Diplopia Detective, a series where we discuss interesting cases of diplopia using both a thoughtful and practical clinical approach. Diplopia is a complex problem that can have a broad spectrum of possible causes. It often requires a detective-like approach to rule out the more dangerous pathologies that could be at play. By being a diplopia detective and systematically evaluating these patients, eye care providers are capable of making challenging, critical, and potentially life saving diagnoses.
CASE REPORT
A 39-year-old African American female was referred to the eye clinic by her primary care physician with a complaint of persistent blur following an injury to the left side of her head one month prior. Her ocular history was remarkable for bilateral LASIK five years earlier without complications. Her medical history was remarkable for stable bilateral tinnitus related to military service, well controlled hypertension treated with hydrochlorothiazide, elevated body mass index (BMI) >40 with a recent weight gain of about 35 pounds, and use of oral contraceptives.
As reported by the patient, she experienced a mild blunt trauma by hitting her head on a cabinet when leaning over to pick up an object off of the floor. She denied loss of consciousness but remembered “seeing stars” and recovered within minutes. Five days following the injury, the patient was seen at a local emergency department due to the onset of visual discomfort and blur, which the patient presumed was related to trauma. The emergency department ran computerized tomography (CT) of the head without contrast which was read as normal, and the patient was diagnosed with post-concussion syndrome. According to our thorough history, she reported that the blur and visual discomfort did not onset immediately at the time of the head trauma, but evolved in the days following. This explained her delayed presentation to the emergency department five days after the injury. Upon further questioning, she also reported persistent low grade bilateral photophobia and headache that had not changed since her visit to the emergency department, one month prior to visiting the eye clinic. She denied worsening of her established tinnitus or other new neurological symptoms.
During her ocular evaluation, it was determined that the patient’s interpretation of blur was actually horizontal diplopia which worsened when looking to the left side. This was explained by a left-sided abduction deficit, with all other extraocular muscle movements (EOMs) being full. Abduction was 60% in the left eye with full range on forced duction test, consistent with a cranial nerve VI (abducens nerve) palsy. The rest of the ocular and facial nerve examination was unremarkable, including CN V testing with cotton swab prior to forced duction test. Intraocular pressure was measured at 16 mmHg in the right eye and 18 mmHg in the left eye by iCare rebound tonometry. Her visual acuity was corrected to 20/20 in each eye, confrontation visual fields were normal, and pupillary response was normal without afferent pupillary defect. Posterior segment evaluation and optical coherence tomography (OCT) of the optic nerve head revealed bilateral low grade optic disc edema, left greater than right (Figures 1 and 2). Formal 24-2 Humphrey visual field (HVF) testing was unremarkable in each eye (Figure 3).

Figure 1. OCT Optic Nerve showing subtle edema of the optic discs bilaterally.

Figure 2. Fundus photography with evidence of subtly blurred optic disc margins, left eye (B) greater than right eye (A), characteristic of mild optic disc edema.

Figure 3. 24-2 Sita Fast Humphrey Visual Field without significant visual field defects corresponding to cavernous sinus meningioma.
At this point, post concussion syndrome was deemed an inadequate diagnosis, as the patient was experiencing persistent EOM dysfunction and with clinical signs of more significant intracranial pathology. The presence of optic disc edema raised concern for conditions causing an increase in intracranial pressure. Traumatic extraocular muscle entrapment could not be conclusively ruled out without a dedicated orbital scan, although this was also less likely with a clinically negative forced duction test. The patient’s elevated BMI, young female demographic, recent weight gain, and use of oral contraceptive suggested idiopathic intracranial hypertension (IIH) with associated left abducens nerve palsy as a more likely preliminary diagnosis. As part of a comprehensive evaluation for this and other possible intracranial causes, Magnetic Resonance Imaging (MRI) of the brain and orbits with dedicated cuts through brainstem, and Magnetic Resonance Venography (MRV) with and without contrast were ordered.
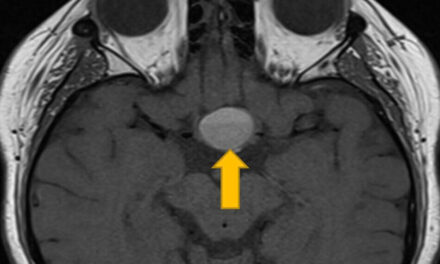
MRI and MRV, done 2 weeks following the initial ocular exam, revealed a homogeneously enhancing extra-axial mass along the left cavernous sinus with a dural tail and thickening along the left tentorium cerebelli. There was also encasement of the left cavernous internal carotid artery with mild narrowing and partial extension into the sella (Figure 4). The mass measured roughly 1.7 by 1.2 centimeters axially (Figure 5). The patient was ultimately diagnosed with a cavernous sinus meningioma causing left sixth cranial nerve palsy. Subsequent referral to and evaluation by neurosurgery resulted in successful treatment with a single session of Gamma Knife radiosurgery.

Figure 4. T1 weighted coronal MRI showing a left cavernous sinus meningioma wrapped around the left internal carotid artery.

Figure 5. T1 weighted axial MRI highlighting the size of the meningioma, measured at roughly 1.7 mm by 1.2 mm.
At follow-up four months post radiation, the patient retained 20/20 vision in the right and left eye with full visual field testing bilaterally. She had nearly 80% abduction of the left eye which had improved from 60% at presentation. There was limited potential to regain completely full extraocular motility based on residual tumor and duration of cranial nerve impingement. Dilated fundus exam showed improvement in optic disc edema bilaterally, with minimally elevated disc margins in the left eye only. The patient remained actively under care of the neurosurgeon, and was scheduled for a follow up in 3 months with her care team for monitoring and repeat treatment if indicated.
DISCUSSION
The cavernous sinus is a crucial anatomical structure located on either side of the sella turcica in the base of the skull. It serves as a complex network of venous channels responsible for draining blood from various regions of the brain and face, and plays a vital role in intracranial pressure regulation.1 It is closely associated with the oculomotor, abducens, and trochlear nerves, as well as the ophthalmic and maxillary division of the trigeminal nerve.1,2 Due to its central location and proximity to several cranial nerves, the integrity of the cavernous sinus is crucial for maintaining proper cerebral function, facial sensation, and eye movement.
Ophthalmoplegia is one of the most common symptom manifestations of cavernous sinus lesions, along with proptosis, chemosis, Horner’s syndrome, exophthalmos, and either pain or loss of sensation of the face.3,4 This relationship of the cavernous sinus to numerous cranial nerves should make it a top consideration when evaluating any diplopia case. This is even more imperative for patients with multiple cranial nerve involvement. Observational studies show that 25-37% of cases involving multiple cranial nerves were associated with cavernous sinus pathology.5,6 In this specific case, the findings of abducens palsy without other cranial nerve involvement, mild disc edema and persistent symptoms were inconsistent with the initial diagnosis of post concussion syndrome. Cranial nerve VI palsy presents less frequently from head trauma without associated increase in intracranial pressure.7 Concomitant risk factors and clinical findings suggestive of more significant intracranial disease prompted the need for further work up.
In the evaluation of cavernous sinus neoplasms, either MRI or CT can be performed. An MRI (specifically T1 weighted MRI) is generally more informative than CT, as it is able to offer greater enhancement of soft tissue, making it ideal for lesions such as meningiomas.3,8 Moreover, MRI does not use radiation which makes it safer for repeated imaging. MRI is better suited to establish a relationship between a lesion and surrounding structures like cranial nerves and the internal carotid artery.9 When available and feasible, MRI is the preferred form of imaging performed to evaluate cavernous sinus lesions.10 CT scans are faster, more readily available, and are often used initially in emergency situations or when MRI is contraindicated. They are particularly useful for detecting bone abnormalities and calcifications which commonly occur with meningiomas.9,11 Ultimately, in patients with signs of a lesion in the cavernous sinus, both enhanced CT and MRI can be used adjunctively to aid in diagnosis and management.5
Historically, treatment of meningioma required invasive intracranial surgical techniques. Surgical management was frequently met with complications due to close proximity to neurovascular structures and potential for significant neurological deficits.12 Even when full excision was possible, recurrence rates were still in the 18-25% range.13 Gamma Knife radiotherapy was the first available stereo-tactic treatment option for meningioma.12 This targeted radiation is an incisionless procedure, aimed at delivering radiation directly to abnormal tissues in order to stop growth and potentially shrink an existing mass.14 It is now used for both primary treatment in small, poorly surgically accessible tumors (like the one referenced in this case) and as adjunctive treatment to reduce the risk of tumor recurrence following surgical excision.12 A 2015 study of 628 patients with intracranial meningioma showed nearly 95% tumor control rate over five years.15 Gamma Knife treatment is considered a high control, low risk treatment option for cerebral meningioma.12,15
In reviewing the details of this case, it is apparent that multiple errors resulted in a delay of diagnosis and intervention. Her initial symptoms were incorrectly attributed to an unrelated injury, the first physical examination in the emergency department did not detect the abducens palsy, and the primary imaging was improperly interpreted as normal. This is, unfortunately, not uncommon in the diagnostic course of small meningiomas. A study of diagnostic errors of optic nerve sheath meningiomas done in 2019 showed that 20% of missed cases were caused by inaccurate or misinterpreted patient history, 24% were related to missing physical exam findings, and a further 20% were related to inappropriate imaging and/or image interpretation.16 The final take home should be that all exam elements including an: in-depth history, careful physical exam with appropriate ancillary testing, and thorough imaging with careful interpretation are vital elements in solving the mysteries of diplopia.
Clinical pearls for catching the culprit:
- Abducens nerve palsy is the most common cranial nerve palsy in adults.17,18
- Selecting the proper testing is a balancing act of time, cost, and necessity. Thorough imaging and targeted image review can be crucial in identifying potentially life-threatening pathology.
- Imaging protocol for any cranial nerve palsy should follow the minimum accepted guidelines of age <50, pupil involving complete or pupil sparing partial oculomotor nerve palsy, known cancer history, any additional localized signs or symptoms, failure to improve at 1 month, or failure to resolve after 3 months.16,19
References
- Patel CR, Fernandez-Miranda JC, Wang WH, Wang EW. Skull Base Anatomy. Otolaryngol Clin North Am [Internet]. 2016 Feb [cited 2024 Apr 8];49(1):9-20. Available from: https://doi.org/10.1016/j.otc.2015.09.001
- Ngnitewe Massa R, Minutello K, Mesfin FB. Neuroanatomy, Cavernous Sinus. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459244/
- Mahalingam HV, Mani SE, Patel B, Prabhu K, Alexander M, Fatterpekar GM, Chacko G. Imaging Spectrum of Cavernous Sinus Lesions with Histopathologic Correlation. RadioGraphics [Internet]. 2019 May [cited 2024 Apr 8];39(3):795-819. Available from: https://doi.org/10.1148/rg.2019180122
- Hekmatpanah J. Evidence-based treatment of cavernous sinus meningioma. Surg Neurol Int [Internet]. 2019 Nov 22 [cited 2024 Apr 8];10:228. Available from: https://doi.org/10.25259/sni_268_2019
- Sharma P, Mehta M, Garg R, Rizvi I, Verma R, Goel M, Malhotra H, Malhotra K, Kumar N, Uniyal R, Pandey S. The Multiple Cranial Nerve Palsies: A Prospective Observational Study. Neurol India [Internet]. 2020 [cited 2024 Apr 8];68(3):630. Available from: https://doi.org/10.4103/0028-3886.289003
- Keane JR. Multiple Cranial Nerve Palsies. Arch Neurol [Internet]. 2005 Nov 1 [cited 2024 Apr 8];62(11):1714. Available from: https://doi.org/10.1001/archneur.62.11.1714
- Kung N, Van Stavern G. Isolated Ocular Motor Nerve Palsies. Semin Neurol [Internet]. 2015 Oct 6 [cited 2024 Apr 8];35(05):539-48. Available from: https://doi.org/10.1055/s-0035-1563568
- Hirsch W, Hryshko F, Sekhar L, Brunberg J, Kanal E, Latchaw R, Curtin H. Comparison of MR imaging, CT, and angiography in the evaluation of the enlarged cavernous sinus. Am J Roentgenol [Internet]. 1988 Nov [cited 2024 Apr 9];151(5):1015-23. Available from: https://doi.org/10.2214/ajr.151.5.1015
- Bhatkar S, Mahesh KV, Sachdeva J, Goel A, Goyal MK, Takkar A, Ray S, Shree R, Balaini N, Singh P, Singh R, Patnaik SN, Prabhat N, Lal V. Magnetic resonance imaging (MRI) versus computed tomographic scan (CT scan) of brain in evaluation of suspected cavernous sinus syndrome. Neuroradiol J [Internet]. 2020 Dec [cited 2024 Apr 9];33(6):501-7. Available from: https://doi.org/10.1177/1971400920970921
- Park J. Evidence-Based Clinical Decision Support System| UpToDate | Wolters Kluwer [Internet]. UpToDate; 2024 Mar 22 [cited 2024 Apr 8]. Available from: https://www.uptodate.com/contents/epidemiology-pathology-clinical-features-and-diagnosis-of-meningioma?search=meningioma&source=search_result&selectedTitle=1~125&usage_type=default&display_rank=1#H1094512137
- Klinger DR, Flores BC, Lewis JJ, Barnett SL. The treatment of cavernous sinus meningiomas: evolution of a modern approach. Neurosurg Focus [Internet]. 2013 Dec [cited 2024 Apr 9];35(6):E8. Available from: https://doi.org/10.3171/2013.9.focus13345
- Lippitz BE, Bartek J, Mathiesen T, Förander P. Ten-year follow-up after Gamma Knife radiosurgery of meningioma and review of the literature. Acta Neurochir [Internet]. 2020 Jun 26 [cited 2024 Apr 9];162(9):2183-96. Available from: https://doi.org/10.1007/s00701-020-04350-5
- Agrawal D, Naik V, Pahwa B, Singh M, Kale S. Correlation Based on the WHO Grading with Tumor Control and Clinical Outcome Following Gamma Knife Radiosurgery in Meningiomas. Neurol India [Internet]. 2023 [cited 2024 Apr 9];71(7):140. Available from: https://doi.org/10.4103/0028-3886.373628
- Chen C, Chapman P. Evidence-Based Clinical Decision Support System| UpToDate | Wolters Kluwer [Internet]. UpToDate; 2022 Apr 5 [cited 2024 Apr 9]. Available from: https://www.uptodate.com/contents/stereotactic-cranial-radiosurgery#H14
- Jang CK, Jung HH, Chang JH, Chang JW, Park YG, Chang WS. Long-Term Results of Gamma Knife Radiosurgery for Intracranial Meningioma. Brain Tumor Res Treat [Internet]. 2015 [cited 2024 Apr 9];3(2):103. Available from: https://doi.org/10.14791/btrt.2015.3.2.103
- Kahraman-Koytak P, Bruce BB, Peragallo JH, Newman NJ, Biousse V. Diagnostic Errors in Initial Misdiagnosis of Optic Nerve Sheath Meningiomas. JAMA Neurol [Internet]. 2019 Mar 1 [cited 2024 Apr 8];76(3):326. Available from: https://doi.org/10.1001/jamaneurol.2018.3989
- Graham C, Gurnani B, Mohseni M. Abducens Nerve Palsy. [Updated 2023 Aug 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482177/
- Srimanan W, Panyakorn S. Retrospective Analysis of Factors Related to the Long-Term Recovery of Third, Fourth, and Sixth Cranial Nerve Palsy with Etiologies and Clinical Course in a Tertiary Hospital. Clin Ophthalmol [Internet]. 2024 Feb [cited 2024 Apr 8];Volume 18:441-50. Available from: https://doi.org/10.2147/opth.s449127
- Murchison AP. Neuroimaging and Acute Ocular Motor Mononeuropathies. Arch Ophthalmol. 2011;129(3):301. Accessed May 8, 2024. https://pubmed.ncbi.nlm.nih.gov/21402985/

Dr. Carr is a 2016 PCO graduate and completed residency in 2017 at the Wilmington VA Medical Center in Wilmington, DE. She returned on staff in Wilmington in 2019 and is now the student externship coordinator. She has an affinity for all things ocular disease, especially glaucoma, retinal disease, and neuro.

Dr. Beharie completed his BS in Biology with a Neuroscience minor from St. Mary's College of Maryland in 2020. He then recieved his Doctor of Optometry degree from the Accelerated Scholars program at the Pennsylvania College of Optometry in 2024. He is currently practicing at the Visionworks in Waldorf, MD.



{kind=link}