




Ocular Findings in a Patient with Type 1 Myotonic Dystrophy: A Case Report

 Save as PDF
Save as PDFABSTRACT
INTRODUCTION
Myotonic dystrophy is a complex genetic neuromuscular disorder which affects skeletal and smooth muscle in the eye, heart, endocrine and central nervous system. The ocular manifestations of this condition can present as Christmas tree cataracts, ptosis, dry eye, epiretinal membranes and corneal edema.
CASE REPORT
The patient in this case report who had been diagnosed with myotonic dystrophy type 1 presented with both anterior and posterior segment findings. The objective of this report is to highlight the diagnostic evaluation, management, and clinical implications of the ocular manifestations associated with myotonic dystrophy, and to emphasize the importance of multidisciplinary care in addressing the complex needs of these patients.
CONCLUSION
This case underscores the significance of understanding and recognizing ocular manifestations in the context of myotonic dystrophy, as well as the challenges and opportunities for optimizing patient care in this population.
Keywords: myotonic dystrophy, ocular manifestations, multidisciplinary management
INTRODUCTION
Myotonic dystrophy (DM) – the most common form of muscular dystrophy – is a complex genetic disorder characterized by muscle weakness, myotonia (delayed relaxation of muscles), and multisystem involvement.1 It is inherited as an autosomal dominant trait and is divided into type 1 (DM1) and type 2 (DM2).1 The global prevalence of DM is variable from 0.37 to 36.29 cases per 100,000.2,3
DM1 is diagnosed through evaluation of the patient’s medical history, family history, physical examination and molecular genetic testing of the dystrophia myotonica protein kinase (DMPK) gene on chromosome 19 where the CTG repeat length exceeds 34 repeats.2 Clinical manifestations typically occur when a patient has 50 or more CTG repeats in the DMPK gene.2 Patients display characteristic findings such as atrophy of the neck, face, hands and distal legs.2 The systemic manifestations include distal muscle weakness such as grip myotonia and arm weakness, along with cardiac conduction abnormalities, respiratory muscle weakness and/or mild to moderate cognitive impairment.3 Ocular manifestations are common in myotonic dystrophy, with progressive ptosis being a prominent feature that can significantly impact visual function and quality of life.2,3 Other ocular findings include the formation of Christmas tree cataracts before the age of 50, lower intraocular pressure, Fuchs’ endothelial corneal dystrophy (FECD) and reticular maculopathies.3
Treatment and management of DM1 should be monitored by a multidisciplinary team including an eyecare provider, primary care physician, neuromuscular specialist, physical therapist, speech therapist, neuropsychologist, pulmonologist, cardiologist and genetic counselor.3 Since there is no cure for DM1 at this time, the treatment for these patients focuses on managing their presenting symptoms.3
Ptosis, or drooping of the upper eyelid, in patients with DM1 results from weakness or dysfunction of the levator palpebrae superioris muscle, which is innervated by the oculomotor nerve.4 While ptosis can occur in various neurological and neuromuscular disorders, its association with myotonic dystrophy underscores the importance of recognizing ocular manifestations in the context of this complex genetic condition.4 There are several classifications of ptosis divided into five types of congenital and acquired causes of ptosis: neurogenic, myogenic, mechanical, aponeurotic and traumatic. Myogenic ptosis is most commonly associated with DM1 due to the progressive muscle wasting of the levator muscle.4 The levator weakness can lead to incomplete eyelid closure which can be associated with dry eye signs and symptoms.
This case report discusses a patient with myotonic dystrophy presenting with bilateral ptosis, epiretinal membranes, early Christmas tree cataracts, and peripheral pigmentary changes. The objective of this report is to highlight the diagnostic evaluation, management, and clinical implications of ocular manifestations in myotonic dystrophy, emphasizing the importance of multidisciplinary care in addressing the complex needs of these patients.
CASE REPORT
A 49-year-old female presented for an oculoplastic consultation due to bilateral ptosis secondary to myotonic muscular dystrophy Type 1 (adult-onset), which was confirmed with blood work and PCR (Polymerase Chain Reaction) genetic testing per patient history. The patient complained of ocular dryness, which was worse in the morning, and a mild decrease of vision in both eyes. The patient’s medical history included dry eye syndrome, asthma, prediabetes, hypertension, first-degree heart block, and uterine fibroids. Medications include albuterol sulfate 90 mcg inhaler, losartan 50 mg once daily orally, and Premarin 0.45 mg tablets once daily orally. Surgical history included a pacemaker implantation and hysterectomy. The patient’s daughter had also been diagnosed with DM1.
The best-corrected distance visual acuity with Snellen acuity was 20/25 in the right eye and 20/30 in the left eye. Extraocular motilities and confrontation fields with finger counting were full. Pupils were both significantly miotic with brisk reactivity. During Amsler grid testing, the patient reported paracentral metamorphopsia in both eyes. Intraocular pressure was 11 mmHg in the right eye, and 10 mmHg in the left eye with iCare tonometry. The external ocular evaluation revealed bilateral ptosis (Figure 1), reduced blink rate, incomplete lid closure, and reduced frontalis function.

Figure 1. External photo showing bilateral ptosis.
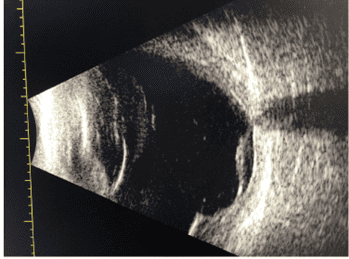
The slit lamp examination revealed inferior punctate staining, reduced Schirmer and reduced tear break-up time in both eyes and a positive Korb Blackie light test which showed an incomplete inferior lid seal. Margin-to-reflex distance testing (MRD) and levator function revealed an MRD1 (upper lid margin to pupillary reflex) of 0.5 mm on the right and 1.0 mm on the left, with a levator function of 9 mm on both sides. Oxymetazoline hydrochloride ophthalmic solution 0.1% was instilled in both eyes, which resulted in a 1.5 mm elevation of her right upper lid margin and a 2.0 mm elevation of the left eye upper lid margin 5 minutes after instillation. The dilated fundoscopic examination revealed mild peripheral anterior cortical changes with early signs of a Christmas tree-like cataract in both eyes,bilateral epiretinal membranes, and a pseudohole in the right eye, both confirmed by optical coherence tomography (OCT) of the macula (Figures 2 and 3). There were also scattered areas of peripheral pigmentary degeneration and tortuosity of the blood vessels in both eyes (Figures 4 and 5). The optic nerve head of both eyes was distinct and pink with a cup-to-disc ratio of 0.40 right eye and 0.40 left eye.

Figure 2. OCT scan of the right eye. The epiretinal membrane caused the formation of a pseudohole.

Figure 3. OCT scan of the left eye. The epiretinal membrane has caused mild traction and led to cystic spaces in the inner retina’s nasal portion.

Figure 4. Fundus photo of the right eye showing peripheral pigmentary changes, as depicted by the white arrow.

Figure 5. Fundus photo of the left eye showing peripheral pigmentary changes, as depicted by the white arrow.
This patient was seen in concert with an oculoplastic surgeon and agreed that a surgical reconstruction would not be ideal since the patient will likely require another surgical intervention in the future due to the progressive nature of DM1. The patient was prescribed oxymetazoline hydrochloride ophthalmic solution 0.1% instilled once a day in both eyes to be used as needed to improve the ptosis, 0.05% cyclosporine instilled twice per day in both eyes and was recommended to apply ointment with mineral oil and white petrolatum once at night in both eyes with lid taping or a sleeping mask. The patient was instructed to return in two months for a follow-up in order to re-evaluate her symptoms, measure the ptosis and re-evaluate the ocular surface with fluorescein staining and Schirmer testing. At her follow-up visit, she reported a significant improvement in her dry eye symptoms with our recommended treatments. She reported that she was not using the oxymetazoline hydrochloride ophthalmic solution 0.1% and as a result, the examination revealed no change in the ptosis. However, there was significant improvement in her tear break up time and Schirmer testing. The inferior superficial punctate keratitis was resolved. She was advised to continue with the 0.05% cyclosporine twice per day, lubricating ointment and lid taping at night in both eyes.
DISCUSSION
Myotonic dystrophy (DM), also known as Steinert’s disease, is an autosomal dominant genetic disorder characterized by myotonia, muscle weakness, and multisystem involvement.5 There are two types: DM1 is caused by expansion of CTG trinucleotide repeats in the DMPK gene on chromosome 19. DM2 is less common than DM1 and caused by abnormal expansion of DNA in the ZNF9 gene on chromosome 3 and has a later age of onset with a milder clinical presentation compared to DM1.6 Genetic testing uses saliva or blood to run a polymerase chain reaction (PCR) which can detect alleles with up to 100-150 CTG repeats or Southern Blot testing which can detect alleles with greater than 150 CTG repeats.6 Higher numbers of CTG repeats have been correlated with an earlier onset of disease and more severe clinical presentation.6 Other tests that may be helpful in the diagnosis are an electromyogram (EMG) and a creatine kinase (CK) blood test if DM1 is suspected in a patient with muscle weakness.6
In addition to its systemic manifestations, DM can present with ocular manifestations that can involve both the anterior and posterior segments. These include ptosis, dry eye, ophthalmoplegia, cataracts, pigmentary retinal changes, and Fuchs’ corneal dystrophy.6
Ptosis, as observed in our patient, results from weakness or dysfunction of the levator palpebrae superioris muscle, which is innervated by the oculomotor nerve (cranial nerve 3).7 There are other etiologies for bilateral progressive ptosis such as myasthenia gravis. In office techniques to aid differential diagnosis include the ice pack test and prolonged upgaze testing to evaluate for early fatigue of the levator muscle. Additional blood work for myasthenia gravis includes testing for acetylcholinesterase receptor (ACh) antibodies and muscle-specific tyrosine kinase (MuSK) antibodies. In myotonic dystrophy, muscle weakness may be progressive and asymmetric which contributes to the functional impairment and aesthetic concerns for affected individuals. A medication that can be used to improve the cosmetic appearance of ptosis is oxymetazoline hydrochloride ophthalmic solution 0.1%.8 This medication is sympathomimetic and an alpha-agonist that causes vasoconstriction which leads to the contraction of the Müller’s muscle lifting the eyelid.8
Christmas tree cataracts are a well-documented finding that is the most common feature of DM and occurs in 100% of patients over the age of 50.9 They appear as refractile multicolored lenticular opacities and are a hallmark sign of DM1. They are thought to be caused by increased concentration of cysteine causing crystallization associated with elevated lens calcium levels.9 If younger patients present with Christmas tree cataracts as the only ocular sign, it warrants genetic testing and blood work to determine if the patient has DM.9 These cataracts are usually not visually significant but can progress and lead to visual impairment.9 Posterior subcapsular cataracts may also occur, but are more common in DM2 than DM1 and tend to warrant cataract extraction due to a higher likelihood of visual impairment.9 The pathogenesis of cataracts in myotonic dystrophy may involve factors such as oxidative stress, altered protein metabolism, and lens fiber abnormalities.9,10 If a patient develops cataracts and is interested in cataract extraction, proper precautions are needed in the operating room due to cardiac and endocrine issues. DM patients are very sensitive to muscle relaxants along with opioids and have a higher risk for cardiac arrhythmias. The anesthetic of choice is ropivacaine HCL due to successful anesthetic outcomes with a rapid onset but minimal cardiac effects. After cataract extraction and intraocular lens placement, there is an increased risk of posterior capsular opacification and anterior capsular phimosis.9 Since the material of most modern mono-focal intraocular lenses are hydrophobic acrylic, these intraocular lenses have been found have a decreased risk of anterior capsular contraction and posterior capsular opacification formation.9
Additionally, patients with myotonic dystrophy may experience abnormalities in ocular motility including ophthalmoplegia, restricted eye movements, and gaze palsy.11 These neurological deficits result from muscular weakness affecting extraocular muscles and involvement of the cranial nerve brain nuclei, but this is a rare finding that usually only occurs in advanced disease.11
In the cornea, DM1 is associated with Fuchs’ endothelial corneal dystrophy (FECD) via RNA-mediated toxicity.12 FECD has an incidence of 36% to 46% in patients with DM1. Monitoring patients with pachymetry and endothelial cell counts with specular microscopy is crucial, especially when the patient is being evaluated for cataract extraction.12
In the retina, DM may be associated with pigmentary changes. This may include butterfly-like macular changes, reticular pigmentary changes in the periphery, or polygonal pigmentary changes in the periphery.13 Fundus autofluorescence can monitor for pigmentary retinal changes over time as any hyper- or hypofluorescence will indicate any changes in the function of the RPE.
There have been reported associations with increased macular thickness and formation of epiretinal membrane (ERM) in patients with DM1 when compared to control patients.14,15 The pathophysiology of ERM formation in patients with DM1 remains unclear.14,15 But since there is a known association, it is recommended that patients diagnosed with DM1 undergo a baseline OCT of the macula to evaluate for any early ERM formation and to monitor for progression as an ERM may also contribute to reduced vision in patients with DM1.
Currently, frontalis sling, levator advancement, brow suspension, and blepharoplasty are the recommended surgical oculoplastic options offered to patients with DM to correct their ptosis.16 Correcting the ptosis of patients with DM can be challenging due to its progressive nature, so it is important to tailor the approach based on the specific needs and conditions of the patient. A comprehensive assessment by an oculoplastic surgeon, in collaboration with other specialists managing DM1, is essential to determine the most appropriate and effective treatment strategy for ptosis in individuals with DM1. Additionally, postoperative care and follow-up are necessary to monitor outcomes and address any potential complications.
CONCLUSION
Patients with DM1 can present with multiple complex ocular findings such as cataracts, dry eye, corneal dystrophies, ptosis, and epiretinal membranes. This case emphasizes the management and factors to consider when managing patients with DM1. For undiagnosed cases of myotonic dystrophy, optometrists can order genetic testing and blood work to aid in the diagnosis of this condition. Optometrists play an important role in managing this condition by managing dry eye symptoms and utilizing medications such as oxymetazoline hydrochloride ophthalmic solution 0.1% to manage ptosis since surgical techniques are relatively contraindicated due to the progressive nature of the condition. Myotonic dystrophy requires a multidisciplinary approach and early identification to ensure patients receive proper care. Continuing research in the pathophysiology of these ocular manifestations and treatment modalities will further enhance the care and quality of life for patients living with myotonic dystrophy.
Take away points
- Myotonic dystrophy is one of the most prevalent forms of muscular dystrophy that is associated with muscle weakness, myotonia and multiple systemic findings.
- Understanding the pathophysiology behind patients’ ocular manifestations of myotonic dystrophy such as ptosis, epiretinal membrane, Fuchs endothelial corneal dystrophy and Christmas tree cataracts is important for managing these ocular conditions and patient symptoms.
- Multidisciplinary management of patients with myotonic dystrophy is essential to preserving quality of life due to the progressive nature of the disease.
REFERENCES
- Vydra DG, Rayi A. Myotonic dystrophy. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557446/
- Diagnosis and management of myotonic dystrophy type 1. JAMA: the journal of the American Medical Association. 2024;331(14). doi:10.1001/jama.2024.2511
- Liao Q, Zhang Y, He J, Huang K. Global prevalence of myotonic dystrophy: An updated systematic review and meta-analysis. Neuroepidemiology. 2022;56(3):163-173. doi:10.1159/000524734
- Shahzad B, Siccardi MA. Ptosis. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546705/
- Lee JE, Cooper TA. Pathogenic mechanisms of myotonic dystrophy. Biochem Soc Trans. 2009 Dec;37(Pt 6):1281-6. doi: 10.1042/BST0371281. PMID: 19909263; PMCID: PMC3873089.
- Bird TD. Myotonic dystrophy type 1. 1999 Sep 17 [Updated 2021 Mar 25]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews. Seattle (WA): University of Washington, Seattle; 1993-2024. https://www.ncbi.nlm.nih.gov/books/NBK1165/
- Kang MJ, Yim HB, Hwang HB. Two cases of myotonic dystrophy manifesting various ophthalmic findings with genetic evaluation. Indian J Ophthalmol. 2016 Jul;64(7):535-7. doi: 10.4103/0301-4738.190157. PMID: 27609169; PMCID: PMC5026082.
- Bacharach J, Lee WW, Harrison AR, Freddo TF. A review of acquired blepharoptosis: prevalence, diagnosis, and current treatment options. Eye (Lond). 2021;35(9):2468-2481. doi:10.1038/s41433-021-01547-5
- Moshirfar M, Webster CR, Seitz TS, Ronquillo YC, Hoopes PC. Ocular features and clinical approach to cataract and corneal refractive surgery in patients with myotonic dystrophy. Clin Ophthalmol. 2022 Aug 25;16:2837-2842. doi: 10.2147/OPTH.S372633. PMID: 36046572; PMCID: PMC9422984.
- Papadopoulos, C., Kekou, K., Xirou, S. et al. Early onset posterior subscapular cataract in a series of myotonic dystrophy type 2 patients. Eye. 32, 622–625 (2018). https://doi.org/10.1038/eye.2017.280
- Thiriez C, Vignal C, Papeix C, Yaici S, Vidailhet M, Roze E. Ophthalmoplegia as the presenting muscle-related manifestation of myotonic dystrophy. Rev Neurol (Paris). 2010 May;166(5):538-41. doi: 10.1016/j.neurol.2009.12.004. Epub 2010 Jan 25. PMID: 20092863.
- Winkler NS, Milone M, Martinez-Thompson JM, Raja H, Aleff RA, Patel SV, et al. Fuchs’ endothelial corneal dystrophy in patients with myotonic dystrophy, type 1. Invest Ophthalmol Vis Sci. 2018 Jun 1;59(7):3053-3057. doi: 10.1167/iovs.17-23160. PMID: 30025114; PMCID: PMC6005624.
- Kimizuka Y, Kiyosawa M, Tamai M, Takase S. Retinal changes in myotonic dystrophy. Clinical and follow-up evaluation. Retina. 1993;13(2):129-35. PMID: 8337494.
- Kersten, H.M., Roxburgh, R.H., Child, N. et al. Epiretinal membrane: a treatable cause of visual disability in myotonic dystrophy type 1. J Neurol. 261, 37–44 (2014). https://doi.org/10.1007/s00415-013-7141-6
- Abed, E., D’Amico, G., Rossi, S., Perna, A., Bianchi, M. L. E., & Silvestri, G. Spectral domain optical coherence tomography findings in myotonic dystrophy. Neuromuscular disorders: NMD. 2020. 30(2), 144–150. https://doi.org/10.1016/j.nmd.2019.11.012
- Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg. 2003 May-Jun;27(3):193-204. doi: 10.1007/s00266-003-0127-5. Epub 2003 Aug 21. PMID: 12925861.

Dr. Canellos is a full-time faculty member of SUNY State College of Optometry. She is an Associate Clinical Professor, Instructor of Record of the Fourth Year Program and the Director of the University Eye Center’s Referral Service. She supervises interns and residents in the Anterior Segment/Cataract clinics of the Advanced Care Service.

Daniel Kowalsky Moskaliuk is currently an optometrist who is practing at Memorial Sloan Kettering Cancer Center in the Ophthalmic Oncology Department. He is a diplomate of the American Board of Optometry, and has an interest in dry eye research and managing ocular toxicities associated with new targeted cancer therapies.

Dr. Bass is a Distinguished Teaching Professor and a 45-year member of the faculty at the SUNY College of Optometry. She is an attending in the Retina and Electrodiagnostic Clinic and Residency Supervisor of the SUNY Residency in Ocular Disease.



{kind=link}