




Retinopathy Prompting Laboratory Testing: a report of two cases

 Save as PDF
Save as PDFAbstract
Background
Often, the presentation of retinopathy can be a telltale sign of underlying systemic pathology. Many times, the retinopathy is consistent with an existing systemic diagnosis. Occasionally, a dilated fundus examination reveals retinopathy not explained by an existing systemic diagnosis.
Case Reports
Presented are a pair of case reports detailing the use of laboratory testing ordered in response to retinopathy. In each case, the retinopathy presentation guided the laboratory tests ordered. In case 1, the known systemic co-morbidities did not explain the type of retinopathy. Therefore, laboratory testing was implemented to explain the etiology of the retinopathy and there in revealing a life-threatening systemic disease (multiple myeloma). Case 2 gives the account of laboratory testing confirming the etiology of the specific retinopathy presentation (lipemia retinalis) and thereafter used as a guide to the effectiveness of systemic treatments.
Conclusion
When presented with such cases, laboratory testing, directed by the retinopathy appearance and patient demographics, can serve as an indispensable method of discovering or confirming systemic disease.
Keywords: retinopathy, laboratory testing, multiple myeloma, pancytopenia, lipemia retinalis, triglyceride
Background
Optometrists are commonly confronted by the challenge of determining the systemic etiology of retinopathies. Often, retinopathy appearance is pathognomonic for a particular systemic disease. Other times, the underlying cause of retinopathy is more complicated to ascertain. Patients may have multiple systemic conditions that can explain the retinal presentation, or they may not yet have any existing systemic etiologic factors. Laboratory testing, directed by the presence of retinopathy, can serve as an indispensable method of discovering or confirming systemic disease.
Case 1: Multiple Myeloma
A 75-year-old white male established patient presented to the clinic for an annual follow-up examination to monitor meibomianitis that was adequately treated with daily lid hygiene and artificial tear use as needed. In addition to good ocular comfort, the patient reported stable vision except for occasional floaters without flashing lights or loss of peripheral vision. The pertinent medical history included anemia and osteoarthritis treated with cholecalciferol and vitamin-mineral supplements. Ocular history was negative for past ocular surgeries or injuries. Upon examination, pupil testing, extraocular movements (EOM), and confrontation visual fields (CVF) were all normal OD and OS. Best corrected acuities were 20/20 OD and OS and slit-lamp examination (SLE) was unremarkable with resolved meibomianitis noted. Intraocular pressures (IOP) measured 17 mmHg OD and 18 mmHg OS. Dilated fundus examination (DFE) revealed vitreous floaters and dot-blot hemorrhages along the superior temporal and inferior temporal vascular arcades OU.
Due to the absence of diabetes or hypertension diagnosis, the etiology of the bilateral retinal hemorrhaging was initially unclear at the time of this examination. The pre-existing diagnosis of anemia and the patient’s age prompted the ordering of the following laboratory tests: Hemoglobin A1C (HbA1c), erythrocyte sedimentation test (ESR), C-reactive protein (CRP), lipid panel, and complete blood cell count (CBC). A carotid ultrasound was requested and revealed no significant stenosis of the right internal carotid artery (ICA) and a 50-69% stenosis of the left ICA. The lipid panel was normal, HbA1c and blood glucose were mildly elevated at 6.9% and 124 mg/dL, respectively. Both ESR and CRP were elevated at >120 mm/hr (reference range of 0 to 20 mm/hr) and 8.1 mg/L (reference range of 0 to 4 mg/L), respectively. The CBC laboratory results confirmed anemia with a red blood cell count of 1.85 per uL (reference range of 4 to 6 per uL), including a critically low hemoglobin (HGB) level of 6.7 g/dL (reference range of 13.5 to 17 g/dL), but also uncovered evidence of leukemia (WBC of 1.76 per uL, reference range of 4 to 10 per uL) and thrombocytopenia (HCT of 21.1%, reference range of 41 to 50%).
As a result of the pancytopenia (a combination of anemia, leukemia, and thrombocytopenia), along with the critically low hemoglobin, the laboratory results were communicated to an emergency room (ER) physician one day following the optometry examination. The patient was telephoned to inform him of the laboratory results and advised that he present to the ER for further evaluation, and the patient agreed to do so. Upon reporting to the ER, the patient reported worsening fatigue and shortness of breath, exacerbated during exertion. Blood pressure measured 159/84 mmHg. ER laboratory results confirmed pancytopenia, including a critically low HGB4 level of 6.9 g/dL. Lab testing also discovered a plasma cell concentration of 85%, consistent with multiple myeloma. To increase hemoglobin levels, two units of packed red blood cells (PRBC) were administered. A head-brain computed tomography (CT) discovered mild periventricular microvascular infarcts. Serum protein electrophoresis (SPEP) showed the presence of a monoclonal protein, also consistent with multiple myeloma.1 CT-guided needle bone marrow aspiration of the iliac bone confirmed the diagnosis of multiple myeloma. The patient was scheduled with an oncologist three days after being discharged from the ER when treatment was initiated with lenalidomide (Revlimid) and dexamethasone.
Four months after first presenting to the optometry clinic with retinal hemorrhages, the patient returned for follow-up. Since his last eye examination, the patient expressed less fatigue and shortness of breath. The patient’s last HbA1c had increased to 11.2%. Subsequently, he was diagnosed with diabetes and treated with glipizide and metformin. The patient conveyed stable vision, good ocular comfort and compliance with medications. Corrected vision measured 20/25- OD and 20/20 OS. Pupil testing, extraocular motility, and CVFs remained normal. Slit-lamp examination remained unremarkable and IOP had increased to 21 mmHg OU. Dilated fundus examination detected less retinal hemorrhaging OD and resolution of retinal hemorrhaging OS.
Discussion: Case 1
Multiple myeloma is a bone marrow cancer causing plasma cell dyscrasia.1,2 As a result, anemia (low RBC), leukemia (low WBC), and thrombocytopenia (low platelets) can all ensue, with anemia being the most common finding.1 Thus, individuals with multiple myeloma suffer from fatigue, weakness, and lethargy (anemia); increased risk of infection (leukemia); and increased risk of bleeding (thrombocytopenia), including retinal hemorrhaging and cerebral vascular accidents. 1,2,3 In addition to pancytopenia, multiple myeloma disrupts osteoblast and osteoclast function, leading to osteopenia.1 Consequences of osteopenia consist of bone and joint pain, osteoporosis, and high blood calcium levels (hypercalcemia).
Multiple myeloma can culminate in a wide range of signs and symptoms. Consequently, there is frequently a significant delay in diagnosis from the onset of symptoms compared to other cancers.4 Discovering the cause of the associated maladies depends predominately on laboratory testing. This patient had an established diagnosis of anemia and osteoarthritis, but only after the laboratory test results, preempted by the presence of bilateral retinal hemorrhaging, was multiple myeloma uncovered. The blood characteristics consistent with multiple myeloma for this individual included pancytopenia (including the hemoglobin critical level prompting the ER visit) and high level of plasma cells1. While the elevated C-reactive protein is of little benefit to investigating multiple myeloma, the elevated erythrocyte sedimentation rate is a confirmatory result.4 This patient’s multiple myeloma diagnosis was likely made in the earlier stages of the disease as his calcium levels repeatedly measured normal, and hypercalcemia is described as a finding of multiple myeloma in its later stages.4 Ergo, in this case, the retinopathy served as an early indicator of multiple myeloma.5
Treatment options for multiple myeloma include chemotherapy, immunomodulators, steroids and monoclonal antibodies, among others.1 Considering medication adverse side effects, disease stage, and concomitant diagnoses, a combination of these drugs is regularly used to manage this disease.1 In the case presented, the patient reported feeling much better following treatment with an immunomodulator, lenalidomide (Revlimid), and dexamethasone. Regrettably, both of these drugs can have significant side effects. This patient was prescribed sulfamethoxazole/trimethoprim and acyclovir as immunomodulators can abbreviate the body’s immune response.1 As lenalidomide (Revlimid) increases the risk of blood clotting, fish oil was added in addition to the patient’s aspirin.1,6 Another possible side effect of lenalidomide is nausea, for which the patient was prescribed ondansetron.7 Optometrists are acutely aware of the possible complications with steroids, and, unfortunately, this patient was not exempt. Ranitidine was given to combat acid reflux, and, as noted above, the patient was diagnosed and treated for diabetes after starting steroid treatments. Additionally, this patient developed ocular hypertension, repeatedly measuring greater than 29 mmHg OU. Subsequent glaucoma testing revealed evidence of glaucoma, leading to treatment with latanoprost. The patient eventually developed bilateral cataracts, secondary to long-term steroid use, and underwent successful cataract extraction OU.
This case is an example of the necessity of laboratory testing used to determine the underlying cause of retinopathy in the absence of a pre-existing explanatory disease. A diagnosis of multiple myeloma was elucidated by the laboratory test results and additional confirmatory testing. Treatment efficacy was monitored via subsequent laboratory testing. While treatment effectively managed the patient’s multiple myeloma, that same treatment resulted in diabetes, glaucoma, and cataracts. Thus, the patient required continued ocular disease care.
Case 2: Lipemia Retinalis
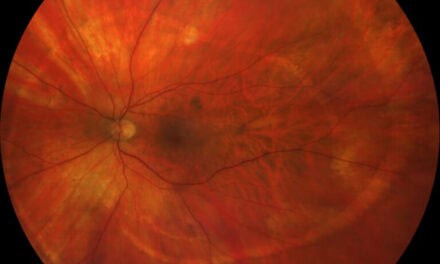
A 59-year-old black male presented to the optometry clinic to evaluate an atypical retinal lesion OD and bilateral white-colored retinal vessels, both evident on diabetic screening fundus photographs two months earlier. The patient had no visual or ocular comfort complaints and reported compliance with systemic medications. The patient’s medical history included insulin-dependent diabetes (last HbA1c of 6.6%), hypertension (blood pressure measured 134/78), and hyperlipidemia (lipid panel discussed below). The patient’s ocular history was positive for non-proliferative diabetic retinopathy and ocular hypertension OU. Pupil testing, CVF, and EOM were normal OD and OS. Visual acuities measured 20/25+ OD and 20/20 OS. Intraocular pressures measured 23 mmHg OD and 24 mmHg OS, and slit lamp examination was noncontributory. Dilated fundus examination revealed normal optic nerve head (ONH) appearance OU and lipemia retinalis, including lipid exudation OD and focal ischemia OS (figure 1). The ocular hypertension was monitored without treatment as the ONH appearance was non-glaucomatous and stable in appearance compared to previous stereo ONH photographs OU with retinal nerve fiber layer thicknesses consistently measured within normal limits OU. Central corneal thickness was measured 601 um OD and 596 um OS, and anterior chamber angles were open to ciliary body OU. Lipid panel results are as follows: low HDL of 16 mg/dL (reference range of 35-80 mg/dL), normal LDL of 46.21 mg/dL (reference range of 10-100 mg/dL), and extremely elevated triglycerides of 6082 mg/dL (reference range of 30-150 mg/dL). The patient’s primary care team, cardiologist, clinical pharmacy specialist, and clinical dietician were alerted to the optometry examination and laboratory test results.

Figure 1. Lipemia retinalis demonstrated by creamy salmon coloration of retinal arteries and veins OU, lipid exudation superior-temporally and superior-nasally to the ONH OD, and a cotton wool spot superior-temporally to ONH OS.
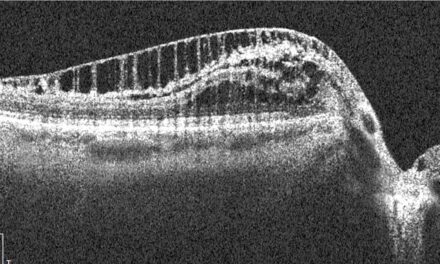
The patient returned to the optometry clinic eight months later, reporting no change in vision or ocular comfort, and continued compliance with medications and follow-ups with other health care specialties. According to the most recent testing, triglyceride levels dropped to 1827 mg/dL; however the HbA1c had increased to 12.7%. Visual acuities held steady at 20/25 OD and OS, and pupil testing, CVF, EOM, and slit-lamp examination remained normal OD and OS. Intraocular pressures were 24 OD and 22 OS, and DFE revealed diminished signs of lipemia retinalis OU (Figure 2).

Figure 2. Significantly reduced salmon coloration of retinal vasculature OU, resolving lipid exudation OD and nearly resolved cotton wool spot OS, compared to baseline photos.
Discussion: Case 2
Lipemia retinalis results from considerably elevated triglyceride levels (>1,000 mg/dL).8,9,10 The consequent retinopathy presents with a creamy salmon coloration of the retinal vasculature, beginning peripherally and progressing posteriorly.8,9,10 Triglycerides are the primary lipids in very-low-density-lipids (VLDL) and chylomicrons.8 The creamy salmon appearance of the retinal vasculature is a visualization of the high blood-chylomicron concentration.9 Retinal lipid exudation and focal ischemia can materialize due to the blood’s hyperviscosity and stunted oxygen-carrying capacity.10 While vision is seldom impacted, lipemia retinalis implies an elevated risk of atherosclerosis that can lead to vasculopathies such as coronary artery disease, carotid stenosis, and cerebral vascular accidents.8,11 Likewise, lipemia retinalis is associated with a heightened threat of pancreatitis which contributes to or negatively impacts diabetes.2,8 Treatment for lipemia retinalis consists solely of addressing the systemic etiology of grossly elevated triglyceride levels.8 The patient must also be educated to stop smoking and substantially limit alcohol intake when applicable.8,11 It is prudent to involve a dietician in the patient’s care to discuss an appropriate diet. Furthermore, the management of this pathology ought to involve the expertise of primary care, cardiology, and clinical pharmacology to develop an adequate exercise regimen, perform medication reviews to limit drugs that can increase cholesterol (i.e. beta-blockers, diuretics, glucocorticoids), and prescribe pharmaceuticals to lower triglycerides (i.e. nicotinic acid and fibric acid derivatives).8,11 Resolution of lipemia retinalis is expected with receding triglyceride levels, with normalized retinal vascular appearance starting posteriorly and proceeding peripherally.8
Conclusion
A comprehensive retinal evaluation guiding appropriate laboratory testing is a powerful tool for revealing systemic pathologies. Undoubtedly, certain diseases require more investigative efforts than others. Regardless, utilizing the combination of retinopathy and laboratory testing can serve as a method of diagnosing and monitoring disease response to treatment.
References
- American Cancer Society: cancer.org
- Rodgin SG. Retinopathy of blood dyscrasias. J Am Optom Assoc 1993 Nov; 64(11):769-779
- Kaiser PK, Friedman NJ, Pineda II R. The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology, 2 ed. Sauders; 2004:314-316
- Koshiaris C, Van den Bruel A, Oke JL, et al. Early detection of multiple myeloma in primary care using blood tests: a case-control study in primary care. Br J Gen Pract 2018 Sep; 68(674): e586-e593. doi: 10.3399/bjgp18X698357
- Lam LA, Rodger DC. Bilateral macular detachments, venous stasis retinopathy, and retinal hemorrhages as initial presentation of multiple myeloma: a case report. Retin Cases Brief Rep 2014 Fall; 8(4):240-4. doi: 10.1097/ICB.0000000000000110
- Block RC, Abdolahi A, Smith B, et al. Effects of Low-Dose Aspirin and Fish Oil on Platelet Function and NF-kappaB in Adults with Diabetes Mellitus. Prostaglandins Leukot Essent Fatty Acids 2013; 89(1):9-18. doi: 10.1016/j.plefa.1013.03.005
- drugs.com
- Alexander LJ. Ocular signs and symptoms of altered blood lipids. J Am Optom Assoc. 1983;54:123-126
- Bowling B. Kanski’s Clinical Ophthalmology: A Systematic Approach. 8th Elsevier; 2016:574
- Rymarz E, Matysik-WoYniak A, Baltaziak L, Prystupa A, Sak J, Grzybowski A. Lipemia retinalis – an unusual case of visual acuity deterioration. Med Sci Monit 2012; 18(8): CS72-CS75. doi: 10.12659/MSM.883257
- National Cholesterol Education Program: NIH Publication No. 01-3670. 2001

Dr. Lee is a 2006 Southern College of Optometry graduate and completed his residency in Primary Eye Care the following year at the Memphis VAMC. He is an AAO Fellow and ABCMO certified. Dr. Lee has been an attending optometrist at the Jackson CBOC since 2009.


{kind=link}