




Guess the Disease: When the Great Masquerader Unveils Its Disguise

 Save as PDF
Save as PDF
Case Presentation
A 49-year-old white man presented to the eye clinic due to sudden-onset scotoma in the right eye. The scotoma was inferior to fixation. He noticed it after exercising and taking a shower the morning prior. He reported having fatigue since last year.
Patient History
Ocular History: Unremarkable
Medical History: Unremarkable
Social History: IV drug use, sober for 10 years; denies sex with men; isolated instance of unprotected sex with an unfamiliar female one year prior
Medication: None
Entrance Testing
Entering Visual Acuity:
OD: 20/25
OS: 20/20
Confrontation Visual Field: Full-to-finger counting, each eye
Pupils: Direct and consensual responses without afferent pupillary defect
Extraocular muscles: Smooth and unrestricted in all directions of gaze, each eye
Anterior Segment Examination

Posterior Segment Examination

Diagnostic Images

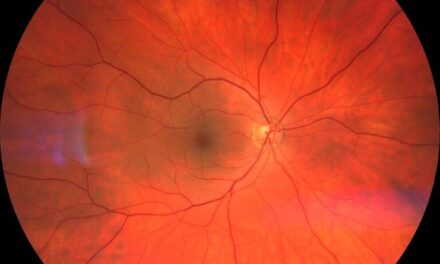
Figure 1. In the right eye, the creamy lesion extended from the optic nerve superior temporally into the macula and along the superior arcades. The inferior and temporal border of the lesion was distinct, with less distinction at the superior and nasal borders.

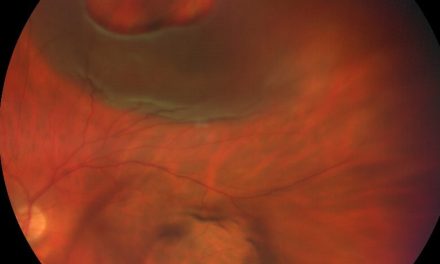
Figure 2. The lesion was nasal to the optic disc in the left eye. Only the superior border of the lesion in the left eye was distinct.
OPTOS Fundus Autofluorescence (FAF)

Figures 3+4. The fundus autofluorescence (FAF) showed increased autofluorescence of the lesions in both eyes (OU). The borders of the lesion were better visualized on FAF than color fundus photos.
OCT Macula

Figure 5. OCT showed diffuse loss of the outer ellipsoid zone and nodular irregularity of the retinal pigment epithelium and outer retina OD (green arrows).
Humphrey Visual Field 30-2

Figure 6. There was an absolute defect that extends inferiorly from the horizontal midline OD (Figure 6B) which correlated to the location of the lesion. There was a possible inferior nasal defect OS (Figure 6A) which was not consistent with the location of the lesion.
Fluorescein Angiography
Figure 7. Fluorescein angiography showed late-stage vascular leakage corresponding to the area of the lesion OD

Figure 8. Fluorescein angiography showed late-stage vascular leakage in the nasal lesion OS.
Knowledge Check
1. What are appropriate case history questions to ask the patient?
-
- Have you ever been diagnosed or treated for an STD?
- Are you a man who has sex with men?
- Are you living with or have been tested for HIV?
- Do you recall a chancre or rash (particularly on the palms of hands or soles of feet?)
- All of the above
2. What is the most appropriate diagnosis?
-
- Acute posterior multifocal placoid pigment epitheliopathy (APMPPE)
- Acute Syphilitic Posterior Placoid Chorioretinopathy
- Age-related macular degeneration (AMD)
- Choroidal osteoma
3. What is the most appropriate treatment?
-
- Doxycycline 100 mg taken twice daily by mouth for 14 days
- Prednisone 60 mg taken daily by mouth for 10 days
- Aqueous crystalline penicillin G 18-24 million units per day, administered as 3-4 million units IV every 4 hours, or continuous infusion, for 10-14 days
- Keflex 500 mg taken twice daily by mouth for 14 days
4. True or False: Syphilis is known as the “great masquerader” for its ability to mimic several conditions due to its extensive range of clinical manifestations.
5. Which of the following labs CANNOT be used to monitor disease activity?
-
- Fluorescent treponemal antibody absorption (FTA-ABS)
- Venereal Disease Research Laboratory (VDRL)
- Rapid plasma reagin (RPR)
- Treponema pallidum particle agglutination (TP-PA)
- A and D
6. True or False: Ocular syphilis is neurosyphilis.
7. True or False: Patients diagnosed with ocular syphilis should be tested for HIV. HIV Pre-exposure prophylaxis (HIV PrEP) should be offered if the HIV test is negative.
Diagnosis and Treatment
Based on the placoid lesions and sexual history, the diagnosis was presumed to be Acute Posterior Placoid Syphilitic Chorioretinitis. Laboratory tests were ordered to confirm the diagnosis. The following is a summary of the test results.

The patient was admitted to the hospital for IV penicillin. He received 4 million units of aqueous penicillin G infusion every four hours for 3 days. He was discharged on the fourth day with continuous home infusion therapy. He completed 14 days of treatment.
Follow-Up
The patient has yet to follow up in the eye clinic due to conflicts with his work schedule. Although a formal visual field has not been repeated, the patient noted that the scotoma had resolved via telephone follow-up two weeks after treatment completion.
Discussion
Syphilis is a sexually transmitted disease caused by the Gram-negative spirochete Treponema pallidum.1,2 It is known as the “great masquerader” for its ability to mimic several conditions due to its extensive range of clinical manifestations.1,2 In contrast to most manifestations of ocular syphilis, Acute Syphilitic Posterior Placoid Chorioretinitis (ASPPC) is easily identifiable due to its characteristic pattern of placoid chorioretinitis. It may be the first presenting sign of syphilis, as it was in this case.3
General Characteristics
ASPPC is characterized by the presence of one or more yellowish, ill-defined, placoid lesions that are typically in the posterior pole or mid-periphery of the fundus.4,5 These lesions usually have a faded center and ground-glass pattern of RPE hyperpigmentation.5,6 They can coalesce to become large confluent lesions.6,7 The chorioretinal lesions can be localized, diffuse, or peripheral.3 Chorioretinitis is accompanied by variable amount of vitreous inflammation and can be associated with superficial retinal hemorrhages, retinal vasculitis, optic disc edema, and serous detachment of the RPE.3,6
The most common presenting symptom of ASPPC is the presence of a scotoma, as it was with the chief complaint of the patient presented in this case.8 Symptomatic eyes are significantly more likely to have a scotoma at presentation, disruption of the ellipsoid zone (EZ), and hyper-reflective elevated lesions of the RPE.8 This EZ disruption produces a scotoma in the involved area.6 Elevated hyperreflective lesions of the outer retina and RPE along with disruption of the EZ and RPE-photoreceptor complex as seen by OCT imaging seem to be associated with worse entering visual acuity (VA). After antibiotic treatment, most patients will have complete or near complete recovery of the scotoma and visual acuity. 6
Diagnostic Imaging Techniques
- High-resolution spectral-domain OCT (SD-OCT): OCT has characterized the pathognomonic features of ASPPC.7 There is segmental loss and disruption of the EZ, followed by attenuation of the external limiting membrane (ELM), patches of hypo-reflectivity in the outer nuclear layer (ONL), “nodular irregularity” of the RPE-photoreceptor junction, and punctate hyper-reflective spots in the superficial choroid.4-5,7-9 OCT may also show transient subretinal fluid.2,7,8 After treatment, usually around 26 days after treatment completion, OCT will show complete recovery of the irregular thickening of the RPE and hyper-reflective dots within the outer retina and choroid.2,4 The OCT also usually demonstrates complete resolution of disruption to the EZ and ELM.4
- Fundus autofluorescence (FAF): Areas of increased autofluorescence (AF) with patchy spots of decreased AF, suggesting altered RPE metabolism, can be visualized even before the development of the classic placoid lesions.4 This is often accompanied by tiny punctate spots of increased and decreased AF representing RPE-photoreceptor complex material overlying the RPE.2,4,5 These spots may persist even after treatment, likely due to permanent RPE damage.4 Buildup of outer segments in the subretinal space, due to incomplete phagocytosis, may explain the yellow placoid lesion seen in patients with ASPPC.9
- Fluorescein angiography (FA): The classic hallmark of placoid lesions in ASPPC is the hypofluorescence of the lesions in the early phase and the diffuse broadening of fluorescein in the late phase as the lesions become progressively hyperfluorescent.10 This indicates RPE dysfunction and choriocapillaris hypoperfusion.2 The blend of the hypofluorescence and hyperfluorescence may create a characteristic “leopard spotting” pattern on FA.3 Fluorescent leakage, indicating retinal vasculitis, can occur along with, and even before the development of, the placoid lesions.4 Severe inflammation can result in frosted branch angiitis, affecting both retinal veins and arteries.11 Subclinical papillitis can be detected as hyperfluorescence on FA and may even leak in cases of severe inflammation.12
Pathophysiology
The pathophysiology of ASPPC is not completely understood.2,4,8 ASPPC may occur in those who are immunocompetent and immunocompromised, including HIV positive individuals.2 ASPPC may be a hypersensitivity immune response to the presence of the spirochete, direct infection of T. pallidum of the outer retina, or a single manifestation with different underlying pathophysiological pathways.2,3 It may have both an autoimmune as well as infectious basis in its pathophysiology.2 Although the underlying mechanisms leading to ASPPC are unclear, there should be a low threshold to test for syphilis in patients presenting with ocular inflammation and chorioretinitis, in particular, even if there is spontaneous resolution.2
Serology
Serological tests are currently the most common diagnostic methods to confirm syphilitic infection.12


Ocular syphilis frequently coexists with neurosyphilis.7 The CDC recommends a complete ocular examination in patients with ocular symptoms.13 If the symptoms are isolated to the ocular structures, cerebrospinal fluid (CSF) examination is unnecessary before treatment.13,14 However, if clinical signs or symptoms of neurologic involvement are present, such as meningitis, stroke, cranial nerve dysfunction, or altered mental status, a lumbar puncture should be performed to analyze the cerebrospinal fluid for the presence of T. pallidum. The patient presented in this report declined the lumbar puncture due to the absence of neurologic symptoms. Therefore, neurosyphilis could not be definitively ruled out. Based on the CDC recommendation to treat ocular syphilis and neurosyphilis the same with intravenous aqueous crystalline penicillin G, the patient’s treatment would remain unchanged if he was had been diagnosed with neurosyphilis. 13
Treatment
According to the CDC, the recommended curative treatment is aqueous crystalline penicillin G 18-24 million units per day, administered as 3-4 million units every 4 hours or continuous infusion for 10-14 days.14 The patient presented in this case report was admitted to the hospital to initiate treatment with IV penicillin G. He was discharged on the fourth day with continuous home infusion therapy until he completed the entire 14-day treatment. It is recommended to repeat quantitative nontreponemal test titers after six and 12 months of treatment to ensure adequate response to treatment and assess potential re-infection from subsequent exposure.12,14 Quantitative nontreponemal test titers should decrease fourfold within six months.12 All persons with ocular syphilis and/or neurosyphilis should be tested for HIV at the time of diagnosis. 13,14 If the HIV test result is negative, HIV pre-exposure prophylaxis (PrEP) should be offered.13,14 Proper patient education and a concerted public health effort to promote safe sex practices are crucial in mitigating the spread of disease.
Conclusion
ASPPC represents a rare but distinct ocular manifestation of syphilis. Although the pathophysiology of ASPPC is not completely understood, the timing and characteristics of multimodal imaging findings depict a characteristic pattern of chorioretinal changes. Regardless of the pathogenesis, in the presence of chorioretinal placoid lesions, syphilitic infection should always be considered. Timely diagnosis and antimicrobial treatment are essential to prevent progression to further late-stage disease manifestations. Given that syphilis is treatable and curable, optometrists should be able to identify ASPPC and coordinate prompt treatment to prevent sight-threatening and life-threatening complications of the disease.
Answers to the knowledge check:
- E 2. B 3. C 4. T 5. E 6. F* 7. T
*Ocular syphilis and neurosyphilis can occur at any stage of syphilis. The treatment for ocular and neurosyphilis is the same. However, CSF analysis is required to definitively diagnose neurosyphilis.
References
- World Health Organization (WHO). Syphilis. May 2023. Available at: https://www.who.int/news-room/fact-sheets/detail/syphilis. Accessed May 1, 2024.
- Ormaechea MS, Hassan M, Nguyen QD, et al. Acute syphilitic posterior placoid chorioretinopathy: An infectious or autoimmune disease? Am J Ophthalmol Case Rep. 2019 Mar 8;14:70-73.
- Zamani M, Garfinkel RA. Corticosteroid-induced modulation of acute syphilitic posterior placoid chorioretinitis. Am J Ophthalmol. 2003 Jun;135(6):891-4.
- Wong W, Naing T, Bhargava M, et al. Acute Syphilitic Posterior Placoid Chorioretinitis: Multimodal Imaging and Electrophysiologic Findings Before And After Treatment. Retin Cases Brief Rep. 2021 Nov 1;15(6):662-669.
- Neri P, Pichi F. Acute syphilitic posterior placoid chorioretinitis: when the great mimicker cannot pretend anymore; new insight of an old acquaintance. J Ophthalmic Inflamm Infect. 2022 Feb 22;12(1):9.
- Chen J, Lee L. Posterior placoid chorioretinitis: An unusual ocular manifestation of syphilis. Clin Ophthalmol. 2008 Sep;2(3):669-73.
- Etheridge T, Bowen RC, Raven M, et al. Ocular Syphilis: Clinical Manifestations and Treatment Course. WMJ. 2019 Dec;118(4):191-195.
- Mirzania D, Zacks D, Zhou Y, et al. Clinical Characteristics and Visual Outcomes of Acute Syphilitic Posterior Placoid Chorioretinopathy. Ophthalmology Retina. 2023 Dec, 7(12),1080-6.
- Sidiqi AM, Navajas EV. Spontaneous Improvement of Syphilis Chorioretinitis: Case Report and Review of Literature. Retin Cases Brief Rep. 2020 Spring;14(2):170-173.
- Li M, Yao B, Xu E, et al. Acute syphilitic posterior placoid chorioretinitis in a woman. QJM. 2024 Mar 8:039.
- Franco M, Nogueira V. Severe acute syphilitic posterior placoid chorioretinitis with complete spontaneous resolution: The natural course. GMS Ophthalmol Cases. 2016 Feb 16;6:02.
- Satyaputra F, Hendry S, Braddick M, et al. The Laboratory Diagnosis of Syphilis. J Clin Microbiol. 2021 Sep 20;59(10):e0010021.
- Centers for Disease Control and Prevention (CDC). Sexually Transmitted Infections Treatment Guidelines, 2021. Neurosyphilis, Ocular Syphilis, Otosyphilis.; 2021. Available at https://www.cdc.gov/std/treatment-guidelines/default.htm. Accessed May 1, 2024.
- Centers for Disease Control and Prevention (CDC). Sexually Transmitted Diseases, Syphilis; January 2024. Available at https://www.cdc.gov/std/syphilis/default.htm. Accessed May 1, 2024.

Dr. Kim is the residency coordinator at the Captain James A. Lovell Federal Health Care Center. She is also adjunct faculty at the Illinois College of Optometry.


{kind=link}