




Assessing Risk of Neovascular Sequelae in Central Retinal Vein Occlusion

 Save as PDF
Save as PDF
ABSTRACT
BACKGROUND
Central retinal vein occlusion is a visually devastating condition which presents with intraretinal hemorrhages, cotton wool spots, optic disc edema and macular edema. Macular edema, macular ischemia, and neovascularization are potential sight-threatening sequelae of central retinal vein occlusion.
CASE REPORT
A 59-year-old female presented for follow-up after a left central retinal vein occlusion which had occurred two years prior. She had a history of treatment with intravitreal bevacizumab for macular edema but had been lost to follow-up for approximately one year. At presentation, visual acuity was 20/100 in the left eye; there was a relative afferent pupillary defect and a superior confrontation visual field defect. Examination revealed retinal neovascularization confirmed with optical coherence tomography angiography and the patient was referred to a retinal specialist for evaluation.
CONCLUSION
Differentiation between ischemic and non-ischemic central retinal vein occlusions provides valuable information regarding visual prognosis and risk of neovascular complications. The extent of retinal ischemia and non-perfusion can be assessed using OCT-A imaging, using both high-resolution central macular scans and wide-field montage imaging to look at the superficial and deep capillary plexus. The onset of neovascular sequelae may be delayed by anti-vascular endothelial growth factor therapies for macular edema and may worsen with treatment interruption. Eye care providers should follow patients with ischemic central retinal vein occlusion closely, every one to two months for up to one year following discontinuation or interruption of anti-angiogenic therapies to promote early detection and treatment of neovascular complications.
Key words: central retinal vein occlusion, neovascularization, optical coherence tomography, angiography
INTRODUCTION
Central retinal vein occlusion (CRVO) is the second most common retinal vascular disorder.1,2 CRVO occurs when a retinal vein becomes obstructed at the level of the optic nerve head giving rise to venous stasis with subsequent retinal non-perfusion and retinal ischemia.3 CRVO is characterized by diffuse intraretinal hemorrhages and dilated, tortuous retinal veins, and is divided into two subtypes, ischemic and non-ischemic CRVO based on the degree of retinal non-perfusion.4 The non-ischemic subtype accounts for 81% of CRVO cases, while only 19% of CRVOs are ischemic.5 Release of vascular endothelial growth factor (VEGF) from hypoxic retinal tissue stimulates macular edema and can give rise to neovascularization of the iris, angle, retina or optic disc. Neovascular complications are more likely to occur in cases of ischemic CRVO.6 Posterior segment neovascularization can lead to vitreous hemorrhage, exacerbating vision loss, and neovascular complications are more likely to occur in cases of ischemic CRVO.6 Retinal infarction can additionally cause permanent ischemic damage to inner retinal layers and parafoveal capillaries, giving rise to macular ischemia and reduced visual function.7 In the Beaver Dam Eye Study, the 15-year cumulative incidence of CRVO was 0.5% which increased with age.2,8,9 Numerous systemic and ocular conditions are associated with CRVO including hypertension, diabetes mellitus, prior retinal vein occlusion, and open-angle glaucoma.5,10,11
Current CRVO management strategies focus on addressing the sequelae of CRVO rather than the occlusion itself.12 Intravitreal anti-VEGF, corticosteroids and laser retinal photocoagulation are mainstays of CRVO management.12,13 When neovascularization occurs it should be treated promptly.12,14,15 Changes to visual function following CRVO decrease vision-related quality of life and impact patients’ ability to perform daily activities such as driving, reading and leisure activities.16,17 Psychological and emotional distress is common following CRVO and includes concerns over disease progression, second-eye involvement, and treatment outcomes.16,17 Patients with CRVO may benefit from referral to low vision rehabilitation and psychotherapy services.18
This report presents a case of retinal neovascularization secondary to ischemic CRVO which developed following interruption of intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy for associated macular edema. Prognostic factors for the development of neovascular complications following CRVO and the consequences of anti-VEGF treatment interruptions will be discussed.
CASE REPORT
A 59-year-old female presented to the optometry clinic with a complaint of decreased vision in the left eye with an unremarkable ocular history. Medical history included type 2 diabetes, antinuclear antibody seropositivity, migraines, gastroesophageal reflux disease, and asthma. She denied hypertension and was a non-smoker. Current medications included albuterol, aspirin 81mg, cetirizine, famotidine, ibuprofen, insulin, montelukast, omeprazole, propranolol, semaglutide and ubrogepant.
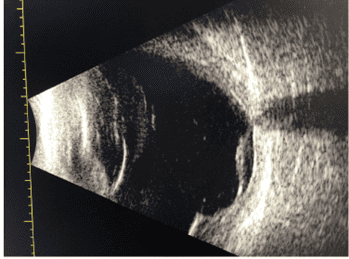
Distance Snellen visual acuity was 20/25 in the right eye and counting fingers in the left eye. No improvement was noted with pinhole in either eye. Extra-ocular motilities were unrestricted in both eyes. Confrontation visual fields revealed supero-nasal restriction in the left eye and were full to finger count in the right eye. Pupils were equal and round with a grade 3 relative afferent pupillary defect in the left eye. Seated, right arm brachial blood pressure was 117/77 mmHg. Anterior segment examination was unremarkable. Dilated fundus examination of the left eye revealed extensive flame hemorrhages and cotton wool spots in all four quadrants emanating from the optic nerve head (Fig. 1). Dot-blot hemorrhages were noted in the mid-periphery in all quadrants of the left eye. Baseline optical coherence tomography (OCT) in the left eye showcased significant macular edema with a serous neurosensory retinal detachment and partial posterior vitreous detachment (PVD) (Fig. 1). The right eye was unremarkable. The patient was diagnosed with CRVO and was referred to a retinal specialist where treatment with bevacizumab was initiated.

Figure 1. Baseline multimodal imaging. A) Baseline color fundus photography showing extensive flame hemorrhages and cotton wools spots in all four quadrants emanating from the optic nerve head. Dot-blot hemorrhages are noted in the mid-periphery in all quadrants. B) Optical coherence tomography through the macula showing significant macular edema with a serous neurosensory retinal detachment.
The patient was co-managed with a retinal specialist over the following year and received a series of five intravitreal bevacizumab injections in the left eye which resulted in complete resolution of the macular edema. The patient was subsequently lost to follow-up with the retina specialist. She reported that she had stopped attending these appointments against the recommendation of the retinal specialist due to poor visual outcomes despite several treatments.

Figure 2. Optical coherence tomography angiography (OCT-A) 1 year following initial presentation. A) En-face montage OCT-A imaging of the superficial vascular plexus (internal limiting membrane to inner plexiform layer) showing extensive retinal nonperfusion (greater than 10 disc areas) within the inferior retina. B) 3×3 mm en-face OCT-A imaging of the superficial vascular plexus centered at the fovea showing irregularity and enlargement of the foveal avascular zone and significant macular nonperfusion. C) 3×3 mm en-face OCT-A imaging of the deep vascular plexus centered at the fovea showing obliteration of microvasculature. The area of B and C is denoted by the yellow box in A.
Optical coherence tomography angiography (OCT-A) imaging was first obtained one year after initial presentation, at which time the macular edema was resolved. Wide-field montage OCT-A imaging demonstrated significant retinal nonperfusion, greater than 10 disc areas primarily restricted to the inferior retina, which was suggestive of a prior ischemic CRVO (Fig. 2). Imaging of the central macula revealed irregularity and enlargement of the foveal avascular zone and significant macular non-perfusion and obliteration of deep microvasculature.
The patient presented to a follow-up appointment two years after initial presentation without visual complaint. Best-corrected distance Snellen visual acuity was 20/20 in the right eye and 20/100 in the left eye. No improvement was noted with pinhole. A superior confrontation visual field defect and grade 1 relative afferent pupillary defect were noted in the left eye. All other entrance testing was unremarkable. Anterior segment examination was unremarkable with no iris or angle neovascularization. Intraocular pressure was 19 mmHg in the right eye and 18 mmHg in the left eye using iCare tonometry.

Figure 3: Optical coherence tomography (OCT) at the 2-year follow-up. A) OCT through the macula showing inner retinal thinning and disorganization (purple arrows). Partial posterior vitreous detachment is noted. B) OCT along the inferior temporal arcade showing pre-retinal neovascularization (red arrows) along the posterior hyaloid face.
Dilated fundus examination of the left eye revealed venous attenuation and sheathing in the inferior temporal arcade. A pre-retinal neovascular frond was noted along the inferior temporal arcade, and a smaller area of retinal neovascularization was noted approximately 1 disc-diameter inferior to the optic nerve head. Collateralization and telangiectasias were appreciated within the inferior macula. No hemorrhages or cotton-wool spots were noted. There was sectoral pallor of the inferior aspect of the optic nerve head with an optociliary collateral vessel. The right eye was unremarkable.
OCT imaging revealed inner retinal thinning and disorganization, particularly within the inferior macula. The outer retinal layers and the ellipsoid zone appeared intact, with no macular edema (Fig. 3). Pre-retinal neovascularization was noted along the posterior hyaloid face at the inferior temporal arcade. This was confirmed by OCT-A (Fig. 4).
The patient was diagnosed with pre-retinal neovascularization secondary to ischemic CRVO and was referred to the retinal specialist for re-evaluation. The patient was educated regarding the symptoms of vitreous hemorrhage and instructed to return for assessment promptly should these occur. Spectacle correction with impact-resistant lenses was recommended given the patient’s functional monocular status. Unfortunately, the patient was lost to follow-up and final outcomes are not known.

Figure 4. Optical coherence tomography angiography (OCT-A) at 2-year follow-up. A) En-face montage OCT-A imaging of the superficial vascular plexus (internal limiting membrane to inner plexiform layer) showing extensive retinal non-perfusion (greater than 10-disc areas) within the inferior retina. Several motion artifacts can be seen which decreases image quality. B) En-face OCT-A of the vitreoretinal interface (300 µm anterior the internal limiting membrane to internal limiting membrane) showing several pre-retinal neovascular membranes (red arrows). The area of B is denoted by the yellow box in A. C) Co-registered OCT B-scan showing pre-retinal neovascularization. Automated software segmentation of the vitreoretinal interface is shown in pink. Red overlay corresponds to OCT-A flow signal.
DISCUSSION
CRVO is potentially visually debilitating: only 12% of ischemic cases have final visual acuity better than 20/100.1 However, in non-ischemic cases, approximately 83% of patients retain vision better than 20/100.1 The visual field of ischemic CRVO cases is typically characterized by a dense central scotoma with relatively intact peripheral vision.1,19 Vision-threatening complications of CRVO include macular edema, macular ischemia, and neovascularization.1 Among neovascular complications, anterior segment neovascularization occurs more frequently than posterior segment neovascularization.20 In cases of ischemic CRVO, 52% develop iris neovascularization, 39% develop angle neovascularization, and 34% develop neovascular glaucoma within 9 months of initial vein occlusion.20 In contrast, only 10% of ischemic cases develop retinal neovascularization at one year following the initial event.20
Intravitreal anti-VEGF therapies are first-line treatment for CRVO-related macular edema, as was done for this patient.12 The CRUISE trial was the first major randomized clinical trial to solidify the role of anti-VEGF therapies in managing macular edema secondary to CRVO.13 In this study, monthly intravitreal ranibizumab injections provided significant visual acuity improvements which were maintained at one year with pro re nata (PRN) dosing.21 At one year, 50.8% of individuals receiving 0.5 mg ranibizumab and 47% receiving 0.3 mg ranibizumab had gained 15 letters or more.21 After 4 years of follow-up for ranibizumab-treated macular edema, the RETAIN study, an extension the CRUISE trial, found that 43.8% of individuals had complete resolution of intraretinal fluid, and visual acuity after four years of follow-up was comparable to outcomes at the end of the CRUISE trial.22 Ranibizumab maintained an excellent safety profile at four years with no severe adverse events.22 Evidence for the use of aflibercept comes from the COPERNICUS study, in which intravitreal aflibercept therapies resulted in rapid resolution of macular edema with sustained effects up to two years. At six months, 56% of individuals gained 15 letters or more, and 75% had complete resolution of retinal fluid.23 The SCORE 2 study showed that bevacizumab treatment achieved similar outcomes to aflibercept,24 and the efficacy of anti-VEGF treatments as first-line treatment for CRVO-associated macular edema was endorsed by a 2014 Cochrane review.25
When there is an inadequate response to anti-VEGF treatments, intravitreal corticosteroids may be administered.12,13 The GENEVA study, which examined an intravitreal dexamethasone implant, found rapid visual acuity improvements with 40% of patients achieving a 15 letters improvement in visual acuity at six months.26 In a study comparing bevacizumab and ranibizumab to dexamethasone, Chiquet et al. found comparable visual acuity and anatomical outcomes between the two groups at 6 and 12-months.27 However, ocular hypertension occurred approximately seven times more frequently in the dexamethasone group.27 Sharareh et al. examined patients with persistent macular edema following treatment with anti-VEGF agents; with the initiation of dexamethasone treatment, further visual acuity improvement and macular edema resolution was noted.28 Despite these benefits, approximately 60% of patients receiving dexamethasone had elevated IOP which required the use of topical ocular hypotensives.28 As such, intravitreal corticosteroids are typically reserved as second line therapies due to the associated risk of elevated intraocular pressure and cataract formation.13,29
While the goal of anti-VEGF therapies is resolution of macular edema, long-term maintenance may be required in some cases and treatment interruptions can be associated with deleterious effects.30,31 The use of anti-VEGF therapies does not eliminate the risk of neovascular complications; rather, the onset of neovascular sequelae appears to occur later compared to cases that do not receive anti-angiogenic treatments.32-34 In eyes with CRVO lost to follow-up during the course of anti-angiogenic therapies, Yang et al. reported an increased rate of neovascular complications and poorer visual outcomes.30 Hogg et al. found that the median time from last anti-VEGF treatment to neovascular events was 10 months.33 Eye care providers should be aware that the risk of neovascular sequelae persists following discontinuation of anti-VEGF treatment and follow-up periods of close observation, every one to two months for up to one year, is warranted following discontinuation of anti-VEGF treatment.15,32,33
Unfortunately, non-adherence and non-persistence remain issues for effective anti-VEGF therapies.35 Dissatisfaction with treatment outcomes and limited visual recovery is a common emotional stressor, and is a leading reason for treatment non-persistence.16,35 This is consistent with the patient in this case who reported that she had stopped attending appointments with the retina specialist due to a lack of visual improvement. Additional reasons for non-adherence to anti-VEGF therapies include financial burden, other comorbid health conditions, and difficulty arranging and attending appointments.35
In cases of retinal neovascularization, panretinal photocoagulation is indicated.12,14,15 In the absence of neovascular complications however, prophylactic photocoagulation is not typically recommended.14 In a prospective study investigating the efficacy of prophylactic photocoagulation for ischemic CRVO, Hayreh et al. found that prophylactic photocoagulation did not decrease the risk of developing neovascular complications or improve visual acuity.19 However, profound loss of peripheral vision measured using Goldmann perimetry was seen after receiving photocoagulation.19 Even in cases of ischemic CRVO, peripheral visual fields are generally preserved due to greater oxygen perfusion from the choroid into thinner retinal tissue in the peripheral retina.19 Combined with the dense central scotoma already present in most ischemic CRVO cases, profound constriction of peripheral vision following photocoagulation can create a number of challenges for orientation and mobility.19 In the acute phase of neovascular complications, serial intravitreal anti-VEGF injections are often used as adjunct therapy to promote early regression of neovascularization, while photocoagulation provides long-term treatment effect.15,36 In cases of media opacity due to vitreous hemorrhage, anti-VEGF therapies are continued in the interim until photocoagulation is possible.6,36 In the absence of concurrent vision-threatening conditions such as retinal detachment, vitreous hemorrhage is usually observed without surgical intervention, allowing for spontaneous resolution and clearing of the visual axis.6 In cases of non-clearing vitreous hemorrhage persisting for 3 months or more, pars plana vitrectomy should be considered to improve vision and allow for photocoagulation; however, duration of vitreous hemorrhage does not appear to impact visual outcomes.6 When neovascular glaucoma develops, topical hypotensive and surgical intervention including cyclo-ablation should be considered.15
The degree of retinal ischemia is a critical prognostic factor to consider, subdividing CRVO into ischemic and non-ischemic subtypes.1,20,37 Retinal non-perfusion of 10 disc areas or more using fluorescein angiography is a commonly used definition for ischemic CRVO.4 OCT-A is a non-invasive and more readily available test which can provide useful information regarding retinal non-perfusion and macular ischemia, assisting eye care providers in differentiating ischemic and non-ischemic CRVO.38 While fluorescein angiography is currently considered the gold standard, OCT-A shows excellent agreement with fluorescein angiography in assessing retinal non-perfusion.39,40 OCT-A is beneficial in cases when patients have an allergy to fluorescein contrast dye, when extensive hemorrhage blocks fluorescent dye, and when patients or clinicians seek to avoid invasive testing.38,40 OCT-A imaging is additionally advantageous by allowing visualization of blood flow in distinct retinal layers, using segmentation which is typically performed automatically by imaging software systems. In the setting of CRVO, clinicians should pay special attention to the superficial capillary plexus (SCP: inner limiting membrane to inner plexiform layer), the deep capillary plexus (DCP: inner plexiform layer), and vitreoretinal interface (anterior vitreous to internal limiting membrane).41 When acquiring OCT-A images for CRVO, providers should attempt to obtain both wide-field and macular imaging.
Wide-field OCT-A imaging allows for thorough evaluation of overall retinal blood flow and shows excellent agreement with fluorescein angiography.39 Wide-field OCT-A images are generally obtained using a panoramic montage by combining images taken in several gazes including central, superior-nasal, superior-temporal, inferior-nasal and inferior-temporal, typically using a large scan size such as 8×8 mm or 12×12 mm.39 Clinicians should examine both the SCP and DCP to evaluate capillary dropout and retinal non-perfusion.39 This can be used to identify ischemic CRVOs and assess risk of neovascular sequelae by determining the extent of retinal non-perfusion.39 Similar to fluorescein angiography, retinal non-perfusion seen in the SCP and DCP of 10 disc areas or more in the posterior pole can be used to define ischemic CRVO.39,42 Additionally, wide-field OCT-A imaging is useful to identify retinal neovascularization.43 To detect preretinal neovascularization, clinicians should examine the vitreoretinal interface, the area anterior to the internal limiting membrane.43 Flow signal detected at the level of the vitreous is characteristic of retinal neovascularization (Fig. 4C).43
Central macular imaging, typically a high-resolution 3×3 mm scan centered on the fovea, allows eye care providers to assess the integrity of the foveal avascular zone (FAZ).44 Providers should qualitatively assess the size and shape of the FAZ and the pattern of surrounding vasculature.44 In the setting of CRVO, the FAZ is typically enlarged and irregularly shaped, with distortion and tortuosity of surrounding vasculature (Fig. 2B and 2C).44 The DCP is more susceptible to ischemic damage and will typically show greater capillary dropout on OCT-A compared to the SCP.44,45 These changes to FAZ morphology are associated with poorer visual acuity, even with resolution of acute macular edema.44,45 Individuals in which the outline of the FAZ is obliterated in more than two quadrants, such as in the above case, are expected to have poor visual acuity, whereas cases where at least half of the FAZ outline remains intact have a better visual prognosis.46 Additionally, more extensive microvascular alterations to the FAZ occur in the presence of greater peripheral retinal non-perfusion.41,47 As such, significant microvascular alterations at the level of the FAZ can be used to identify patients with greater levels of ischemia and who are at higher risk of developing neovascular complications.41 Specifically, microvascular obliteration in more than half of the 3×3 mm central OCT-A field suggests extensive peripheral non-perfusion.41 These patients should receive wide-field montage OCT-A imaging and should be followed as in cases of ischemic CRVO.
CRVOs which are non-ischemic at presentation may convert to ischemic CRVO during follow-up due to progressive capillary damage.4 This occurs most commonly within the initial four months following acute occlusion, with 15% of patients converting from non-ischemic to ischemic CRVO during this period.4 As such, eye care providers should consider re-evaluation of the level of ischemia using OCT-A at four months follow-up and periodically thereafter in patients initially presenting without significant retinal non-perfusion at initial presentation. In patients with ischemic CRVO, monthly follow-up for the initial six months should be arranged as risk of ocular neovascularization is greatest in the initial six-months following onset of ischemia.4,20,37 Examination should include gonioscopy to detect neovascularization of the angle and careful examination of the posterior segment for retinal or optic disc neovascularization.4 Following this and in the absence of neovascular sequelae, the follow-up interval can be gradually extended to annual examination if the patient’s condition remains stable.4
CONCLUSION
Several prognostic factors can be utilized to evaluate risk of potential complications such as retinal neovascularization following CRVO. Eye care providers should differentiate ischemic and non-ischemic CRVO, as neovascular complications occur more frequently in ischemic phenotypes. This can be done in office with OCT-A, a non-invasive imaging modality which can assist risk stratification and allow assessment of the retinal non-perfusion. Clinicians should obtain high resolution 3×3 mm OCT-A images centered at the fovea to examine microvascular alterations to the FAZ, as well as montage 8×8 mm or 12×12 mm images in five positions of gaze to assess retinal non-perfusion and detect retinal neovascularization, closely examining the SCP and DCP. Patients with significant alterations to the FAZ and greater retinal non-perfusion (greater than 10-disc areas) in the posterior pole should be closely followed to promote early detection and treatment of neovascular sequelae. With the use of anti-VEGF for macular edema, these complications may occur later than typically expected, particularly if treatment is interrupted. As such, close observation every one to two months for up to one year is warranted following discontinuation or interruption of anti-VEGF therapies to allow for earlier detection of neovascular complications. Patients referred for treatment should be honestly educated as to disease prognosis and the importance of continued treatment.
REFERENCES
- Hayreh SS, Podhajsky PA, Zimmerman MB. Natural history of visual outcome in central retinal vein occlusion. Ophthalmology. 2011;118(1):119–2. doi: 10.1016/j.ophtha.2010.04.019.
- Song P, Xu Y, Zha M, Zhang Y, Rudan I. Global epidemiology of retinal vein occlusion: A systematic review and meta-analysis of prevalence, incidence, and risk factors. J Glob Health. 2019;9(1):010427. doi: 10.7189/jogh.09.010427.
- Hayreh SS, Zimmerman MB. Fundus changes in central retinal vein occlusion. Retina. 2015;35(1):29–42. doi: 10.1097/IAE.0000000000000256.
- Natural history and clinical management of central retinal vein occlusion. the central vein occlusion study group. Arch Ophthalmol. 1997;115(4):486–491. doi: 10.1001/archopht.1997.01100150488006.
- Hayreh SS, Zimmerman MB, Podhajsky P. Incidence of various types of retinal vein occlusion and their recurrence and demographic characteristics. Am J Ophthalmol. 1994;117(4):429–441. doi: 10.1016/s0002-9394(14)70001-7.
- Wakabayashi T, Patel N, Bough M, et al. VITRECTOMY FOR VITREOUS HEMORRHAGE ASSOCIATED WITH RETINAL VEIN OCCLUSION: Visual outcomes, prognostic factors, and sequelae. Retina. 2023;43(9):1506–1513. doi: 10.1097/IAE.0000000000003839.
- Lima VC, Yeung L, Castro LC, Landa G, Rosen RB. Correlation between spectral domain optical coherence tomography findings and visual outcomes in central retinal vein occlusion. Clin Ophthalmol. 2011;5:299–305. doi: 10.2147/OPTH.S16253.
- Klein R, Moss SE, Meuer SM, Klein BEK. The 15-year cumulative incidence of retinal vein occlusion: The beaver dam eye study. Arch Ophthalmol. 2008;126(4):513–518. doi: 10.1001/archopht.126.4.513.
- Cugati S, Wang JJ, Rochtchina E, Mitchell P. Ten-year incidence of retinal vein occlusion in an older population: The blue mountains eye study. Arch Ophthalmol. 2006;124(5):726–732. doi: 10.1001/archopht.124.5.726.
- Hayreh SS, Zimmerman B, McCarthy MJ, Podhajsky P. Systemic diseases associated with various types of retinal vein occlusion. Am J Ophthalmol. 2001;131(1):61–77. doi: 10.1016/s0002-9394(00)00709-1.
- Risk factors for central retinal vein occlusion. the eye disease case-control study group. Archives of ophthalmology (1960). 1996;114(5):545–554. https://www.ncbi.nlm.nih.gov/pubmed/8619763.
- Flaxel CJ, Adelman RA, Bailey ST, et al. Retinal vein occlusions preferred practice pattern®. Ophthalmology. 2020;127(2):P288–P320. doi: 10.1016/j.ophtha.2019.09.029.
- Ashraf M, Souka AAR, Singh RP. Central retinal vein occlusion: Modifying current treatment protocols. Eye (Lond). 2016;30(4):505–514. doi: 10.1038/eye.2016.10.
- Hayreh SS. Photocoagulation for retinal vein occlusion. Prog Retin Eye Res. 2021;85:100964. doi: 10.1016/j.preteyeres.2021.100964.
- Nicholson L, Talks SJ, Amoaku W, Talks K, Sivaprasad S. Retinal vein occlusion (RVO) guideline: Executive summary. Eye (Lond). 2022;36(5):909–912. doi: 10.1038/s41433-022-02007-4.
- Prem Senthil M, Khadka J, Gilhotra JS, et al. Understanding quality of life impact in people with retinal vein occlusion: A qualitative inquiry. Clin Exp Optom. 2019;102(4):406–411. doi: 10.1111/cxo.12875.
- Ramin S, Rostami F, Ahmadieh H, et al. Vision-related quality of life in patients with retinal vein occlusion. Int Ophthalmol. 2024;44(1):114–1. doi: 10.1007/s10792-024-02916-1.
- Coday MP, Warner MA, Jahrling KV, Rubin PAD. Acquired monocular vision: Functional consequences from the patient’s perspective. Ophthalmic Plast Reconstr Surg. 2002;18(1):56–63. doi: 10.1097/00002341-200201000-00009.
- Hayreh SS, Klugman MR, Podhajsky P, Servais GE, Perkins ES. Argon laser panretinal photocoagulation in ischemic central retinal vein occlusion. A 10-year prospective study. Graefes Arch Clin Exp Ophthalmol. 1990;228(4):281–296. doi: 10.1007/BF00920049.
- Hayreh SS, Zimmerman MB. Ocular neovascularization associated with central and hemicentral retinal vein occlusion. Retina. 2012;32(8):1553–1565. doi: 10.1097/IAE.0b013e318246912c.
- Campochiaro PA, Brown DM, Awh CC, et al. Sustained benefits from ranibizumab for macular edema following central retinal vein occlusion: Twelve-month outcomes of a phase III study. Ophthalmology. 2011;118(10):2041–2049. doi: 10.1016/j.ophtha.2011.02.038.
- Campochiaro PA, Sophie R, Pearlman J, et al. Long-term outcomes in patients with retinal vein occlusion treated with ranibizumab: The RETAIN study. Ophthalmology. 2014;121(1):209–219. doi: 10.1016/j.ophtha.2013.08.038.
- Heier JS, Clark WL, Boyer DS, et al. Intravitreal aflibercept injection for macular edema due to central retinal vein occlusion: Two-year results from the COPERNICUS study. Ophthalmology. 2014;121(7):1414–1420.e1. doi: 10.1016/j.ophtha.2014.01.027.
- Scott IU, VanVeldhuisen PC, Ip MS, et al. Effect of bevacizumab vs aflibercept on visual acuity among patients with macular edema due to central retinal vein occlusion: The SCORE2 randomized clinical trial. JAMA. 2017;317(20):2072–2087. doi: 10.1001/jama.2017.4568.
- Braithwaite T, Nanji AA, Lindsley K, Greenberg PB. Anti-vascular endothelial growth factor for macular oedema secondary to central retinal vein occlusion. Cochrane Database Syst Rev. 2014;2014(5):CD007325. doi: 10.1002/14651858.CD007325.pub3.
- Haller JA, Bandello F, Belfort RJ, et al. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010;117(6):1134–1146.e3. doi: 10.1016/j.ophtha.2010.03.032.
- Chiquet C, Dupuy C, Bron AM, et al. Intravitreal dexamethasone implant versus anti-VEGF injection for treatment-naïve patients with retinal vein occlusion and macular edema: A 12-month follow-up study. Graefes Arch Clin Exp Ophthalmol. 2015;253(12):2095–2102. doi: 10.1007/s00417-015-2947-9.
- Sharareh B, Gallemore R, Taban M, Onishi S, Wallsh J. Recalcitrant macular edema after intravitreal bevacizumab is responsive to an intravitreal dexamethasone implant in retinal vein occlusion. Retina. 2013;33(6):1227–1231. doi: 10.1097/IAE.0b013e31827c53a0.
- Ford JA, Shyangdan D, Uthman OA, Lois N, Waugh N. Drug treatment of macular oedema secondary to central retinal vein occlusion: A network meta-analysis. BMJ Open. 2014;4(7):e005292–005292. doi: 10.1136/bmjopen-2014-005292.
- Yang K, Liu L, Feng H, et al. Outcomes of eyes lost to follow-up in patients with central retinal vein occlusion who are receiving anti-vascular endothelial growth factor treatment. Ther Clin Risk Manag. 2021;17:489–496. doi: 10.2147/TCRM.S303248.
- Yang K, Feng H, Zhang H. Effects of the COVID-19 pandemic on anti-vascular endothelial growth factor treatment in china. Front Med (Lausanne). 2020;7:576275. doi: 10.3389/fmed.2020.576275.
- DeCroos FC, Todorich B, Alshareef R, et al. Neovascular events in eyes with central retinal vein occlusion undergoing serial bevacizumab or ranibizumab intravitreal injections: A retrospective review. J Ophthalmic Vis Res. 2014;9(4):461–468. doi: 10.4103/2008-322X.150825.
- Hogg HDJ, Talks SJ, Pearce M, Di Simplicio S. Real-world visual and neovascularisation outcomes from anti-VEGF in central retinal vein occlusion. Ophthalmic Epidemiol. 2021;28(1):70–76. doi: 10.1080/09286586.2020.1792937.
- Brown DM, Wykoff CC, Wong TP, et al. Ranibizumab in preproliferative (ischemic) central retinal vein occlusion: The rubeosis anti-VEGF (RAVE) trial. Retina. 2014;34(9):1728–1735. doi: 10.1097/IAE.0000000000000191.
- Shahzad H, Mahmood S, McGee S, et al. Non-adherence and non-persistence to intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy: A systematic review and meta-analysis. Syst Rev. 2023;12(1):92–x. doi: 10.1186/s13643-023-02261-x.
- Sun Y, Liang Y, Zhou P, et al. Anti-VEGF treatment is the key strategy for neovascular glaucoma management in the short term. BMC Ophthalmol. 2016;16(1):150–9. doi: 10.1186/s12886-016-0327-9.
- Hayreh SS, Klugman MR, Beri M, Kimura AE, Podhajsky P. Differentiation of ischemic from non-ischemic central retinal vein occlusion during the early acute phase. Graefes Arch Clin Exp Ophthalmol. 1990;228(3):201–217. doi: 10.1007/BF00920022.
- Nobre Cardoso J, Keane PA, Sim DA, et al. Systematic evaluation of optical coherence tomography angiography in retinal vein occlusion. Am J Ophthalmol. 2016;163:93–107.e6. doi: 10.1016/j.ajo.2015.11.025.
- Glacet-Bernard A, Miere A, Houmane B, Tilleul J, Souied E. NONPERFUSION ASSESSMENT IN RETINAL VEIN OCCLUSION: Comparison between ultra-widefield fluorescein angiography and widefield optical coherence tomography angiography. Retina. 2021;41(6):1202–1209. doi: 10.1097/IAE.0000000000002993.
- An W, Han J. Research progress of UWFFA and OCTA in retinal vein occlusion: A review. Eur J Ophthalmol. 2021;31(6):2850–2855. doi: 10.1177/11206721211027411.
- Seknazi D, Coscas F, Sellam A, et al. OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY IN RETINAL VEIN OCCLUSION: Correlations between macular vascular density, visual acuity, and peripheral nonperfusion area on fluorescein angiography. Retina. 2018;38(8):1562–1570. doi: 10.1097/IAE.0000000000001737.
- Nicholson L, Vazquez-Alfageme C, Patrao NV, et al. Retinal nonperfusion in the posterior pole is associated with increased risk of neovascularization in central retinal vein occlusion. Am J Ophthalmol. 2017;182:118–125. doi: 10.1016/j.ajo.2017.07.015.
- You QS, Guo Y, Wang J, et al. Detection of clinically unsuspected retinal neovascularization with wide-field optical coherence tomography angiography. Retina. 2020;40(5):891–897. doi: 10.1097/IAE.0000000000002487.
- Wons J, Pfau M, Wirth MA, Freiberg FJ, Becker MD, Michels S. Optical coherence tomography angiography of the foveal avascular zone in retinal vein occlusion. Ophthalmologica. 2016;235(4):195–202. doi: 10.1159/000445482.
- Winegarner A, Wakabayashi T, Hara-Ueno C, et al. RETINAL MICROVASCULATURE AND VISUAL ACUITY AFTER INTRAVITREAL AFLIBERCEPT IN EYES WITH CENTRAL RETINAL VEIN OCCLUSION: An optical coherence tomography angiography study. Retina. 2018;38(10):2067–2072. doi: 10.1097/IAE.0000000000001828.
- Mejía ME, Ríos HA, Rosenstiehl S, Rodríguez FJ. Optical coherence tomography angiography as predictor of visual outcomes in retinal vein occlusion treated with antiangiogenic therapy. Eur J Ophthalmol. 2023;33(1):434–440. doi: 10.1177/11206721221099487.
- Cavalleri M, Sacconi R, Parravano M, et al. Optical coherence tomography angiography in central retinal vein occlusion: Macular changes and their correlation with peripheral nonperfusion at ultra-widefield fluorescein angiography. Ophthalmologica. 2022;245(3):275–284. doi: 10.1159/000522503.

Dr. Ethan Wohlgemuth is a graduate of the University of Waterloo School of Optometry and Vision Science. He completed residency at Northeastern State University Oklahoma College of Optometry where he managed a wide variety of complex ocular disease, performed in-office optometric surgical and laser procedures. Dr. Wohlgemuth practices in Ontario, Canada as a full-scope medical optometrist.

Dr. Molly Brawdy is a graduate of the University of Waterloo School of Optometry and Vision Science. They practice in rural northern British Columbia, Canada, providing comprehensive medical eye care.


{kind=link}