




Xerophthalmia in a Child with Autism and Severe Sensory Food Aversion: A Case Report

 Save as PDF
Save as PDFABSTRACT
BACKGROUND
Vitamin A deficiency (VAD) is a cause of preventable blindness worldwide and is considered rare in developed countries. However, several at-risk populations exist, including those with autism spectrum disorder (ASD) with selective eating habits. The ocular manifestations of VAD are collectively termed xerophthalmia and consist of a variety of signs, including conjunctival keratinization and corneal scarring. In severe cases, corneal perforation and permanent vision loss can result. VAD is treated with vitamin A supplementation (VAS), and early intervention is critical to prevent permanent vision loss, in addition to other systemic morbidities.
CASE REPORT
A 5-year-old non-verbal male with ASD presented with chronic bilateral redness, tearing, and discharge for the past several months. Examination of this patient was historically quite difficult due to limited patient cooperation. His clinical signs persisted despite treatment for initial differential diagnoses of bacterial conjunctivitis and chronic allergic keratoconjunctivitis, which led to the expansion of differential diagnoses. VAD became the leading diagnosis when it was revealed that the patient had sensory food aversions leading to a severely limited diet. Diagnosis of VAD was confirmed, and VAS was initiated.
CONCLUSION
This case report demonstrates the importance of xerophthalmia as a differential diagnosis for chronic keratoconjunctivitis in pediatric patients, especially for those with autism who are at an increased risk of sensory food aversions and limited diets.
Keywords: Xerophthalmia, vitamin A deficiency, autism, food aversions
INTRODUCTION
Vitamin A deficiency (VAD) is a major cause of preventable childhood blindness worldwide.1 Poor vitamin A intake manifests as xeropthalmia which can cause corneal clouding and melting (keratomalacia), permanent corneal scarring, and subsequent blindness. VAD has also been linked to an increased risk for anemia, respiratory infections, and increased mortality.2 Despite its rarity in developed nations, VAD can result from selective eating habits, fat malabsorption disorders or liver disease.1
Selective eating habits, or young children being described as “picky eaters,” is not an uncommon occurrence, though they are more frequently demonstrated in children with autism spectrum disorder (ASD).3 ASD is a neurodevelopmental disorder characterized by impaired social behavior, deficits in communication abilities, and repetitive or stereotyped behavioral patterns. Children with ASD tend to struggle with sensory processing and, therefore, are at risk of poorly balanced diets due to hypersensitivity to food texture and consistency.3 A study combining the results of 2102 children with ASD and typical development found that atypical eating behaviors were 15 times more common in those with ASD vs neurotypical children (5%).4 This food selectivity may persist and can sometimes become more pervasive in adults with ASD.5 Selective diets in all patients, both neurotypical and with ASD, can cause multiple nutritional deficiencies, including VAD.3
This case report demonstrates the importance of considering xerophthalmia caused by Vitamin A deficiency in the differential diagnoses for chronic keratoconjunctivitis in pediatric populations, especially for those with autism and sensory food aversions. The presence of non-specific symptoms, such as ocular irritation, redness, and photophobia, along with examination difficulty due to patient cooperation in children with ASD, can often delay appropriate diagnosis and treatment. Timely diagnosis of xerophthalmia and treatment with vitamin A supplementation (VAS) is crucial to prevent permanent vision loss, other systemic morbidities, and early mortality.
CASE REPORT
A 5-year-old non-verbal Hispanic male with ASD presented with a history of chronic bilateral redness, tearing, and discharge for the past several months. The patient had been seen at the clinic four times in the past month for these symptoms. Examination of this patient was historically quite difficult due to limited patient cooperation and photophobia, but the findings became more reliable over time as the patient became more comfortable with being examined. He was previously treated with antibiotic and steroid eye drops for initial differential diagnoses of bacterial conjunctivitis and chronic allergic keratoconjunctivitis, respectively. There was minimal improvement of symptoms with these treatments, which led to further follow-up and the expansion of differential diagnoses.
At this examination, the patient was more cooperative and anterior segment findings revealed bilateral conjunctival xerosis, corneal clouding without staining, and watery discharge (Figure 1). Posterior pole assessment and B-scan ultrasound were unremarkable in both eyes. Bacterial eSwab cultures and a respiratory viral panel were collected, and both were negative.
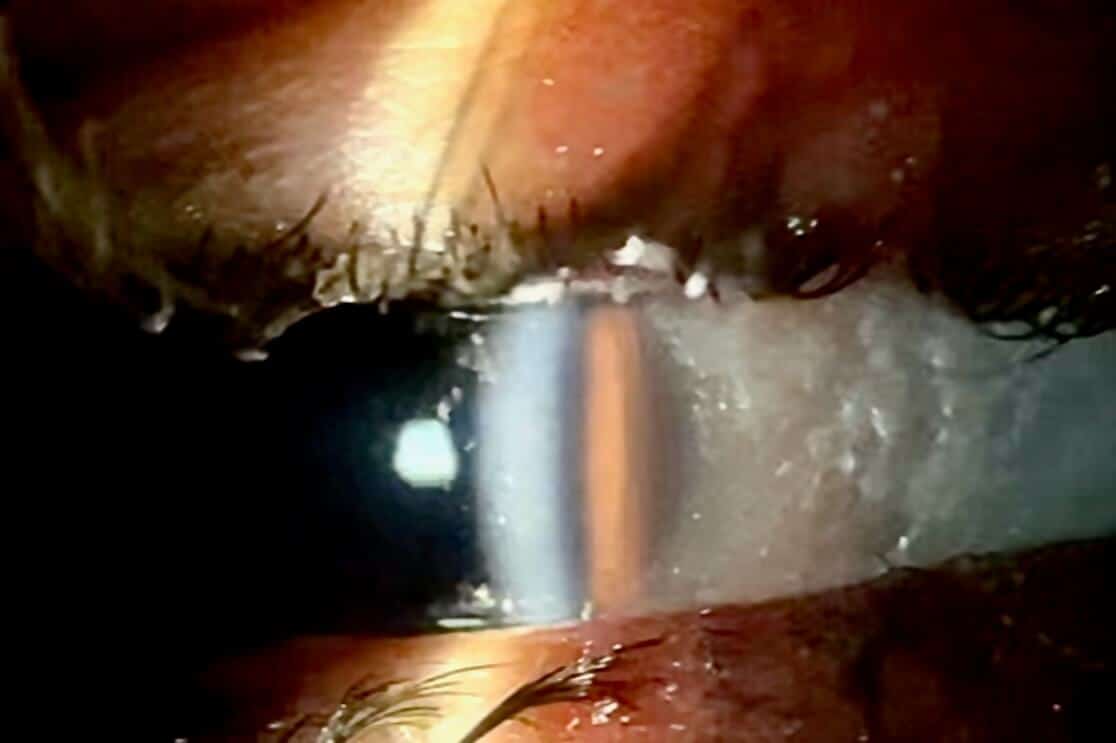
Figure 1. Slit lamp photo at the time of diagnosis, demonstrating conjunctival xerosis and corneal clouding of the right eye
Upon further questioning, the patient’s mother revealed that due to the patient’s severe sensory food aversions, the patient had a very limited diet. His diet consisted of dry cereal, white rice, graham crackers, and fried potatoes. He did not eat meat, fruits, or vegetables and was not taking any multivitamins. Growth chart assessment showed the patient was at the 5th percentile for height and the 25th percentile for weight. The diagnosis of xerophthalmia due to vitamin A deficiency became likely based on the history of the patient’s limited diet and the presence of bilateral conjunctival xerosis and corneal clouding. Serology testing confirmed severe vitamin A deficiency, with vitamin A levels of <5 mcg/dL (normal range 20-43 mcg/dL). Additionally, a comprehensive nutritional evaluation during the inpatient evaluation for poor oral intake revealed iron deficiency anemia, along with deficiencies in vitamins D, K, and B12.
The patient’s care was co-managed by ophthalmology, pediatrics, and hematology. Vitamin A supplementation (10,000 IU daily) was initiated by the pediatrician. Hydrating artificial tears and ointment for the ocular surface were also recommended by ophthalmology. At first, the child’s mother had difficulties administering the VAS at home, and the xerosis of the conjunctiva persisted. Eventually, one month after proper treatment with VAS, the patient’s signs and symptoms of xerophthalmia completely resolved (Figure 2). The pediatrician also prescribed multivitamins, iron, and B12 supplements, and the patient was referred to a feeding and nutrition specialist to address his limited diet.

Figure 2. External photo showing complete resolution of anterior segment signs 2 months after initiation of Vitamin A Supplementation
DISCUSSION
This report highlights the possible ocular complications of VAD in a child with ASD and a severely limited diet. VAD is rare in developed countries, and this fact can lead to delayed diagnosis.1 As demonstrated in this case, nonspecific ocular symptoms in conjunction with examination challenges contribute to diagnostic complexity. Additionally, physicians cannot rely on body mass index (BMI) as an indicator of proper nutrition. An unbalanced diet high in sugars and fats often increases BMI, but patients remain deficient in vitamins and nutrients.6 Vitamin A is acquired mainly from the diet in foods such as liver, eggs, and leafy green vegetables.1 Restrictive diets and food aversions in children can put them at risk of developing VAD.3 With up to 85% of those with ASD manifesting food selectivity and restrictive diets, clinicians managing these patients should inquire about dietary history and initiate further workup if suspicious of deficiencies.5
Both the anterior and posterior segments of the globe require Vitamin A for proper functioning. Ocular manifestations of VAD are collectively known as xerophthalmia and tend to occur in a reliable sequence.7 Xerophthalmia initially manifests as night blindness (nyctalopia), as Vitamin A is a precursor of photopigments and VAD leads to rod photoreceptor dysfunction.1,8 Early ocular surface changes include corneal clouding, conjunctival keratinization, and Bitot’s spots, which are pathognomonic of VAD.7-9 These findings can progress to severe corneal scarring, ulceration, and even perforation without prompt treatment. In a recent case series of six patients with autism and VAD, two patients developed irreversible blindness due to corneal perforation and scarring.10 Late-stage posterior segment manifestations are less common than the anterior segment findings of VAD. Subretinal drusenoid deposits can occur in the macula or periphery.11 Additionally, VAD causes altered bone growth, which can affect the skull and cause narrowing of the optic canals, leading to compression and poor perfusion of the optic nerve. This can be visually devastating, as demonstrated in a case report of a child with autism with VAD who had compression on the optic nerve leading to optic nerve atrophy and permanent blindness.12 In addition to bony overgrowth, other systemic manifestations of VAD include anemia, impaired growth, failure to thrive, and increased susceptibility to infection.8
The recommended daily allowance of Vitamin A for children is 400-900 mcg per day, depending on the child’s age.13 In patients with VAD and xerophthalmia, higher doses of vitamin A are used as treatment to decrease both ocular and systemic complications of VAD. The World Health Organization guidelines recommend 50,000 international units (IU) for children less than 6 months of age, 100,000 IU for children 6-11 months of age, and 200,000 IU for children 12 months of age and older. This dose is given for two days with a third dose after two weeks.1,13 In the case presented, the patient’s pediatrician recommended a long-term VAS of 10,000 IU every three days because the patient was unable to obtain vitamin A from his diet. Patients taking high-dose vitamin A should be monitored for signs of toxicity, including hepatotoxicity, fatigue, and intracranial hypertension.1
Most patients show improvement in ocular surface disease after initiation of vitamin A supplementation. Nyctalopia usually improves within 24-48 hours after initiating VAS. Conjunctival xerosis and Bitot’s spots begin to resolve within two to five days after VAS is initiated and fully resolve in two weeks. If VAS is started before corneal ulceration occurs, the corneal clouding will fully resolve over the course of one week. Partial-thickness ulcers usually heal over time with minimal scarring and without any impact on vision.7 Corneal transplantation can be considered in patients with dense corneal scarring that affects vision, although typically the visual outcome is poor.1 Posteriorly, the subretinal drusenoid deposits take one to four months to resolve.7 Unfortunately, once optic nerve damage occurs, the vision loss is permanent and does not resolve with VAS.12
As previously mentioned, the patient in this case was referred for feeding therapy. Therapy for treating food selectivity in children with ASD has been found to help them overcome their selective eating habits and obtain a more balanced diet.4 As selective eating habits can become more severe in adults with ASD, effective feeding therapy for this population remains an important area of study.5
CONCLUSION
Restrictive diets can lead to vitamin A deficiency and other nutrient deficiencies.1,3 Children and adults with ASD are at increased risk of nutrient deficiencies, as they are more likely to demonstrate selective eating habits.5 In this population, diagnosis of xerophthalmia can be challenging due to the limits of cooperation with examination, as well as the non-specific symptoms, such as ocular irritation, redness, and photophobia. Therefore, clinicians should routinely inquire about dietary history when evaluating those with ASD. Early initiation of vitamin A supplementation in these cases may prevent irreversible vision loss and systemic complications.
REFERENCES
- Song A, Mousa HM, Soifer M, Perez VL. Recognizing vitamin A deficiency: special considerations in low-prevalence areas. Curr Opin Pediatr. 2022;34(2):241–247.
- Wang R, Zhang H, Hu YC, et al. Serum Vitamin A Nutritional Status of Children and Adolescents Aged 6-17 Years – China, 2016-2017. China CDC Wkly. 2021;3(9):189-192.
- Cermak SA, Curtin C, Bandini LG. Food selectivity and sensory sensitivity in children with autism spectrum disorders. J Am Diet Assoc. 2010;110(2):238-246.
- Mayes SD, Zickgraf H. Atypical eating behaviors in children and adolescents with autism, ADHD, other disorders, and typical development. Res Autism Spectr Disord. 2019;64:76-83.
- Pubylski-Yanofchick W, Zaki-Scarpa C, LaRue RH, Manente C, Kahng S. Treatment of Food Selectivity in an Adult With Autism Spectrum Disorder. Behav Anal Pract. 2021;15(3):796-803.
- Calcaterra V, Verduci E, Milanta C, et al. Micronutrient Deficiency in Children and Adolescents with Obesity—A Narrative Review. Children. 2023;10(4):695.
- Smith J, Steinemann TL. Vitamin A deficiency and the eye. Int Ophthalmol Clin. 2000;40(4):83-91.
- Chiu M, Watson S. Xerophthalmia and vitamin A deficiency in an autistic child with a restricted diet. BMJ Case Rep. 2015;2015:bcr2015209413.
- Das S, Chandra A. Bitot Spots: A Pathognomonic Sign of Vitamin A Deficiency. Am J Med. 2023;136(10):e195-e196.
- Marek S, Forbes G, Avery RA, et al. Potential blindness from nutritional xerophthalmia in autistic patients. J AAPOS. 2023;27(4):198.e1-198.e4.
- Levine DA, Mathew NE, Jung EH, et al. Characteristics of vitamin A deficiency retinopathy at a tertiary referral center in the United States. Ophthalmol Retina. 2024;8(2):126-136.
- Cheah JASS, Muhammed J, Tharmathurai S, Hamzah N, Rahmat J. Optic neuropathy in an autistic child with vitamin A deficiency: a case report and literature review. 2022;14(2):e22074.
- Awasthi S, Awasthi A. Role of vitamin A in child health and nutrition. Clin Epidemiol Glob Health. 2020;8(4):1039–1042.

Annmarie Craig, MD is the Chief Ophthalmology Resident at BronxCare Health System. She earned her MD from Wayne State University School of Medicine and completed her undergraduate training at the University of Michigan. Dr. Craig will begin a glaucoma fellowship at NYU Langone Health in July 2026.

Dr. Schaffer completed her Doctor of Optometry degree with a concentration in pediatrics at the New England College of Optometry in 2024. She went on to complete a Pediatric Optometry/Ocular Disease residency at BronxCare Health System in Bronx, NY. Dr. Schaffer currently serves as an attending optometrist at NECO Center for Eye Care Roslindale and as an Assistant Professor of Clinical Optometry at New England College of Optometry.

Alexis Pelowski is a pediatric optometrist at BronxCare Health System and at NYC Health + Hospitals | Metropolitan. She is also the co-supervisor of the BronxCare Pediatric Optometry/Ocular Disease residency program.

Dr. Crane specializes in pediatric optometry. She helped develop and establish the Pediatric Optometry/Ocular Disease Residency program at BronxCare Health System. Dr. Crane is currently an attending optometrist for the Pediatric Optometry/Ocular Disease and Ocular Disease/Primary Care optometry residencies at BronxCare Health System.




{kind=link}