




Multimodal Imaging in the Diagnosis of Solar Retinopathy Secondary to Viewing Solar Eclipse with Inadequate Eye Protection

 Save as PDF
Save as PDFABSTRACT
Solar maculopathy is damage to the central macula secondary to sungazing. There is an increased risk of solar maculopathy following solar eclipses. Younger, emmetropic patients with clear ocular media are at greatest risk of developing this condition. Multimodal imaging and a thorough case history can aid in making the diagnosis. This article reports a case of solar maculopathy in a young patient who viewed the solar eclipse of 2024 with counterfeit eclipse glasses. It covers the use of multimodal imaging in eliminating differentials and supporting the diagnosis, as well as current literature regarding the treatment and management of this rare condition.
CASE REPORT
An 18-year-old Caucasian female presented with complaints of bilateral central scotomas that began shortly after she looked at the solar eclipse. She wore eclipse glasses given to her from an unknown source. Based on her reported clarity of vision through the glasses, these were not dark enough to protect her eyes. Her visual acuity was 20/20-2 in the right eye (OD) and 20/25-1 in the left eye (OS). The diagnosis of solar maculopathy was made based on results from fundus photographs, fundus autofluorescence, visual field, and optical coherence tomography.
CONCLUSION
Multimodal imaging and a thorough case history can aid in the diagnosis of solar maculopathy. OCT and fundus autofluorescence can identify small, focal macular lesions. Solar eclipses present a unique increased risk factor for photic damage of the retina. Providers should be aware of the presentation of solar maculopathy and how it appears on ocular imaging. Before each solar eclipse, there is an increase in public outreach measures regarding the dangers of sungazing, but patients can still be fooled by counterfeit eclipse glasses that only increase the risk of retinal injury. Prevention remains the most effective known treatment. Eye care providers play a vital role in spreading awareness of the dangers of sungazing and in detecting solar maculopathy.
Keywords: solar retinopathy, solar maculopathy, solar eclipse retinopathy, optical coherence tomography, fundus autofluorescence, visual field
INTRODUCTION
Solar retinopathy, also known as solar maculopathy or photic retinopathy, is damage to the outer retina resulting from sungazing. The excessive exposure to sunlight produces photochemical, photothermal, and photomechanical damage to the retinal tissues.1-4 Direct viewing of the sun is never safe for the human eye, and solar retinopathy has been associated with various etiologies, including sungazing as religious practice, due to mental illness or hallucinogen use, or during recreation or military service.1,5-8 There is even a longstanding history of misinformation that sungazing can ‘cure’ refractive error.9
Solar eclipses present a unique temptation to look at the sun for an extended period. Cases of solar retinopathy typically increase shortly after an eclipse.10 Shadowing of the sun makes viewing it more comfortable, but an eclipse is only safe to view without eye protection during the brief totality- when the sun is entirely covered by the moon. When even 1% of the sun is visible, it is intense enough to produce retinal damage.11 Retinal damage can be prevented by using safe viewing practices. Devices like pinhole projectors allow indirect viewing. Direct viewing requires specialized filters that transmit less than 0.003% of visible light and less than 0.5% of near-infrared radiation.11 With less than 0.003% transmission, filters that are safe for viewing of the sun allow little visibility for other tasks and are considerably darker than regular sunglasses. Sunglasses are not sufficient protection for safe sungazing and may in fact increase the risk. The tint promotes mydriasis, allowing more light to enter the eye, and decreases discomfort with solar viewing.8 Damage can occur rapidly: less than one minute of solar viewing with insufficient protection can produce a retinal lesion.2
Reports of unsafe fake and counterfeit eclipse glasses abound in the lead up to an eclipse. While it is difficult to quantify how many unsafe glasses are sold, one manufacturer identified a counterfeit of their product being sold online prior to the April 2024 eclipse. They estimated at least 100,000 of these unsafe, counterfeit glasses were sold before the listing was removed.12-13
This case report describes a patient who developed solar retinopathy after viewing the partial solar eclipse of 2024 with inadequate eye protection. It covers the use of multimodal imaging in eliminating differentials and supporting the diagnosis, as well as current literature regarding treatment and management of this rare condition.
CASE REPORT
An 18-year-old, emmetropic, Caucasian female active-duty Navy patient presented with a complaint of a new-onset “spot” in her central vision of each eye. The spot appeared smaller at distance but seemed larger and more disruptive with near vision. The visual disturbance was constant and stationary.
The patient reported that she viewed the partial solar eclipse three days before this exam. She was given safety glasses of unknown origin by someone at her workplace. Her vision through the glasses was similar to wearing sunglasses, and she was able to walk around comfortably without feeling her vision was significantly impacted by the tint. She viewed the eclipse with these glasses on and reported she also glanced at the sun without any protection. In office, the patient was shown NASA-approved solar eclipse filters, and she stated that they were significantly darker than the tinted glasses she used to view the eclipse. Unlike the glasses she wore while sungazing, the eclipse filters did not allow her to see her environment comfortably. From this description, her glasses during the eclipse could not have been adequately dark and were likely counterfeit.
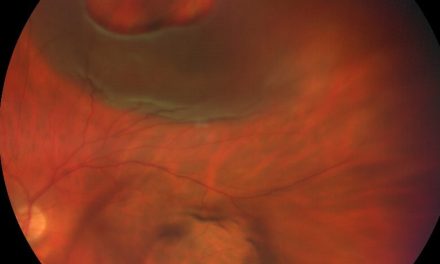
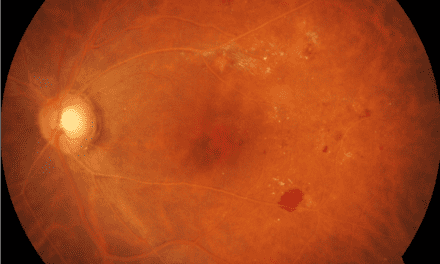
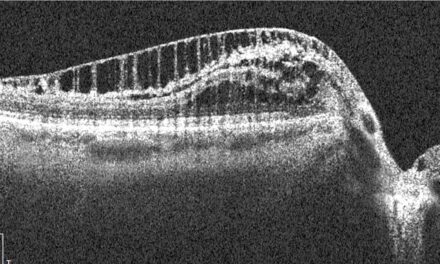
The patient’s entering acuity uncorrected was 20/20-2 in the right eye (OD) and 20/25-1 in the left eye (OS). Entrance testing and anterior segment examination were unremarkable. Dilated fundus examination revealed a focal, yellow-white lesion in the fovea of each eye (Figure 1). Fundus autofluorescence showed minimal foveal hyperautofluorescence in the left eye and was unremarkable in the right eye (Figure 2). Optical Coherence Tomography (OCT) of the macula demonstrated full-thickness, columnar hyperreflectivity in the fovea, with disruption at the junction of the photoreceptor inner segments and outer segments (Figures 3 and 4). These OCT findings were greater in the left than the right eye. The patient underwent 10-2 Humphrey visual field (HVF) testing, which demonstrated shallow focal point defects in each eye (Figure 5).

Figure 1. Color fundus photos showing focal, yellow-white lesion in the fovea of right and left eye.

Figure 2. Fundus autofluorescence showing unremarkable findings OD and subtle, focal hyperautofluorescence of the OS fovea

Figure 3. En Face OCT with hyperreflective lesion with central hyporeflectivity at the level of the IS/OS-Ellipsoid layer in right eye and left eye. The mid-retinal layer also shows a hyperreflective lesion in each eye.

Figure 4. OCT with full-thickness hyperreflectivity and disruption of the IS/OS junction in the fovea of OD (left) and OS (right).

Figure 5. HVF 10-2 imaging of OD and OS, showing non-specific scattered shallow point defects.
Based on the history and findings, the patient was diagnosed with solar retinopathy of both eyes. She was educated about protecting her eyes from the sun and avoiding direct eye contact with the sun. Artificial tears were recommended for comfort. A home Amsler grid was provided, and the patient was educated on its use and to return to the clinic with new or worsening blind spots or metamorphopsia. A follow up was scheduled for the following month.
DISCUSSION
Solar retinopathy is a rare condition characterized by phototoxic damage to the outer retinal layers in the macula. The outermost layer of the retina, the retinal pigmented epithelium (RPE), absorbs most of the solar radiation that reaches the retina and is the site of any photothermal damage. The light-sensitive photoreceptors suffer oxidative photochemical damage.2,14 The most significant cause of maculopathy is photochemical damage.1-2 Patients present with complaints of reduced visual acuity, which can range from 20/20-20/200, and they may also experience central scotoma, metamorphopsia, and dyschromatopsia.15-16 Solar maculopathy is often painless, as the retina has no sensory nerves, but patients may present with periorbital pain. Pain is a rare finding with an unclear etiology. It may occur from corneal superficial punctate keratitis, which can result from intense solar exposure with or without retinal involvement.17
Case history is important to making the diagnosis, but patients are not always forthcoming with a history of sungazing.4,15,18 Multimodal imaging can support the diagnosis and is especially vital in patients who deny sun exposure.
Color images may reveal a yellow-white lesion during the acute phase of solar retinopathy. Later, this lesion becomes reddish and sharply demarcated.15 Fundus autofluorescence (FAF) provides noninvasive imaging of retinal function by showing changes in lipofuscin distribution in the RPE. In phototoxic damage to photoreceptors, hypoautofluorescence results from the death of photoreceptors, while hyperautofluorescence can occur due to accumulation of lipofuscin debris from dying photoreceptors.18-19 In the case above, the FAF findings were subtle while the color images showed more obvious changes. However, in some reported cases, FAF can demonstrate characteristic foveal findings of small areas of hypoautofluorescence surrounded by a hyperautofluorescent ring, especially in cases of chronic solar retinopathy.14,20
Fluorescein angiography (FA) is not generally considered necessary for diagnosing solar retinopathy, but it can help eliminate differential diagnoses in cases where a history of sungazing is not elicited. FA is less sensitive than OCT in detecting subtle macular defects due to photic damage and the images may appear normal or show a window defect at the location of the lesion.1,16,21 A few reports use Optical Coherence Tomography Angiography (OCT-A) to image solar maculopathy lesions. Their results often show normal vasculature but may show enlargement of the deep foveal avascular zone months after presentation.5,22 Further cases with OCT-A imaging are needed to establish its utility in this condition.
OCT of solar retinopathy has characteristic findings. The outer retinal layers are hyporeflective, with loss of the IS/OS photoreceptor junction. Acute cases show columnar hyperreflectivity involving all foveal layers with disruption of the IS/OS junction, though chronic cases and later acute damage resolves to outer retinal hyporeflectivity.15,18,20-22 The RPE regenerates while the postmitotic photoreceptors cannot.21 In chronic solar retinopathy, only photoreceptor defects may be evident, while acute solar retinopathy is more likely to involve both the RPE and photoreceptor layers.4,21 The degree of disruption of the IS/OS junction seen on OCT is correlated to visual acuity and prognosis for recovery.15
Given how focal the damage can be, en face OCT can be helpful to catch small lesions, especially in patients with poor fixation during OCT as the en face report captures a wider area of the retina.19 The en face images of the outer retina will show a ring of hyperreflectivity with central area of hyporeflectivity at the location of the damaged photoreceptors.19,22
Other types of photic damage can mimic solar retinopathy on OCT. Intraoperative exposure to light, such as during cataract surgery, vitrectomy, or other procedures, can result in similar outer retinal damage, but the damaged retinal areas from these etiologies are more likely to be larger and more likely to be juxtafoveal. Damage from exposure to lasers can also damage only the foveal photoreceptors.4 Thus, obtaining a good case history and excluding exposure to other sources of light is important in making a diagnosis of solar retinopathy.
The duration and intensity of exposure to sunlight affect the severity of damage to the retina, but there are several risk factors that make an individual more susceptible to developing solar damage. The cornea and lens absorb much of the ultraviolet (UV) light, particularly short wavelength, high energy UV-C and UV-B rays before it reaches the retina. UV-A, visual spectrum, and infrared light reaches the retina. The lens opacifies with age, further reducing transmission to the retina and protecting the eye from photic damage.2 Younger patients with clear lenses are more prone to solar retinopathy, as their lenses block less light and allow more transmission across the spectrum, including high-energy UV-B light.1-2,4,15,23-24 Pseudophakic patients are not at greater risk than a phakic young adult, as intraocular lenses are standardized to block UV transmission to the retina.25 Emmetropes and low hyperopes are also more prone to damage, as the optics of their eye focus light well into a single point.23 Patients who are taking photosensitizing medications, which include tricyclic antidepressants, tetracyclines, sulfonamides, and some oral contraceptives, are also at greater risk.15 Increased body temperature at time of exposure and light ocular pigmentation are also theorized to contribute.4,15,18 Cases may present as bilateral or unilateral; when bilateral and asymmetric, the dominant eye may be more profoundly affected as patients may close their nondominant eye in response to discomfort.23
No treatment is needed in most cases as recovery is spontaneous. In severe cases, or in cases that do not show significant improvement after several weeks, oral and injected steroid therapy has been used.26-28 The efficacy of these treatments is not established, given few documented cases and that time alone is effective in reducing symptoms. Additionally, the ocular side effects of steroid use are well known, and one case report documents a patient who developed central serous chorioretinopathy after initiation of systemic steroid treatment for solar retinopathy.1,26 Antioxidants have been proposed as a potential treatment or preventative measure to offset the oxidative phototoxicity, but there is little evidence for their efficacy.1,7 Chronic sungazing may contribute to increased risk of developing age-related macular degeneration, and providers may recommend antioxidant supplements in these patients to reduce this future risk.1
The prognosis for solar retinopathy is generally good. The yellow-white acute lesion appears 1-3 days after the initial insult, and fades in 10-14 days to a red, lamellar outer retinal hole.1 The initial appearance is due to edema and release of lipofuscin from damaged cells, which gives way to atrophy of the outer retinal layers.23,15 Vision usually improves over a few weeks or months, and many patients experience significant improvement or resolution of symptoms in 3 to 6 months after the insult.1,23,27 One study found that 80% of patients returned to 20/40 or better visual acuity.29 Another found that 92.3% of patients had “mild or no visual impairment,” defined as 20/70 or better.20 The visual prognosis is worse for chronic sungazers than those with isolated, acute injury such as from looking at an eclipse.1 At 6 months, no further recovery is expected, and most patients retain an outer retinal defect on OCT.24 Those that remain symptomatic can have permanent, often mild, decreased vision and a persistent central scotoma.1,20
CONCLUSION
Multimodal imaging and a thorough case history can aid in the diagnosis of solar maculopathy. The primary diagnostic tests include OCT and fundus autofluorescence, which can identify small, focal macular lesions. Solar eclipses present a unique increased risk factor for photic damage. Providers should be aware of the presentation of solar maculopathy and how it appears on imaging. Before each solar eclipse, there is an increase in public outreach measures regarding the dangers of sungazing, but patients can still be fooled by counterfeit eclipse glasses. Counterfeit glasses increase the risk of retinal injury by promoting mydriasis, comfort, and a false belief that the eyes are protected. Prevention remains the most effective known treatment. Eye care providers play a vital role in spreading awareness of the dangers of sungazing and fake eclipse glasses, and they are the first line in detecting and managing solar maculopathy.
REFERENCES
- Begaj T, Schaal S. Sunlight and ultraviolet radiation-pertinent retinal implications and current management. Surv Ophthalmol. 2018 Mar-Apr;63(2):174-192.
- Glickman R. Ultraviolet phototoxicity to the retina. Eye & Contact Lens: Science & Clinical Practice. 2011 Jul 37(4):p 196-205.
- Mainster MA. Solar eclipse safety. Ophthalmology. 1998 Jan;105(1):9-10.
- Singh SR, Vaidya H, Borrelli E, Chhablani J. Foveal photoreceptor disruption in ocular diseases: An optical coherence tomography-based differential diagnosis. Surv Ophthalmol. 2023 Jul-Aug;68(4):655-668.
- Demirtaş AA, Öncül H. Solar retinopathy from sun gazing under the influence of ecstasy: A longitudinal analysis of OCT and OCTA findings. Photodiagnosis Photodyn Ther. 2021 Sep;35:102359. doi: 10.1016/j.pdpdt.2021.102359. Epub 2021 May 25.
- Devadason DS, Mahmood S, Stanga PE, Bishop PN. Solar retinopathy in a patient with bipolar affective disorder. Br J Ophthalmol. 2006 Feb;90(2):247
- Reddy M, Abhilasha P, Ramachandran AS, Thirunavukarasu M. Solar retinopathy on sun-gazing in mania. Archives of Mental Health. 2018;19(169)
- Rohring V, Rehmani A, Smith E, Smith E, Berg P. Drone retinopathy. J Curr Ophthalmol. 2018 Jul 13;31(1):106-108.
- Albini F, Riva MA. Medicus curat: sungazing versus spectacles? Eye (Lond). 2020 Aug;34(8):1303-1304.
- Ricks C, Montoya A, Pettey J. The ophthalmic fallout in Utah after the great American solar eclipse of 2017. Clin Ophthalmol. 2018;12:1853-1857. Published 2018 Sep 21.
- Chou B. Eye safety during solar eclipses – myths and realities. Z. Madourian & M. Stavinschi (eds.) Theoretical and Observational Problems Related to Solar Eclipses, Proceedings of a NATO Advanced Research Workshop. 1996; 243-247.
- Aziz S. Counterfeit eclipse glasses are selling online. How to spot fakes – national [Internet]. Global News; 2024. Available from: https://globalnews.ca/news/10389637/fake-solar-eclipse-glasses/
- American Astronomical Society warns of Counterfeit & Fake Eclipse Glasses [Internet]. 2024. Available from: https://aas.org/press/american-astronomical-society-warns-counterfeit-fake-eclipse-glasses
- Khatib N, Knyazer B, Lifshitz T, Levy J. Acute eclipse retinopathy: a small case series. J Optom. 2014 Oct-Dec;7(4):225-8.
- Klemencic S, McMahon J, Upadhyay S, Messner L. Spectral domain optical coherence tomography as a predictor of visual function in chronic solar maculopathy. Optometry and Vision Science. 2011 Aug;88(8):p 1014-1019.
- Moran S, O’Donoghue E. Solar retinopathy secondary to sungazing. BMJ Case Rep. 2013;2013:bcr2012008402. Published 2013 Jan 25.
- Billore OP, Shroff AP, Vasavada KA. Superficial keratitis following solar eclipse burn (report of 6 cases). Indian J Ophthalmol. 1982 Jul;30(4):355-6.
- Bruè C, Mariotti C, De Franco E, Fisher Y, Guidotti JM, Giovannini A. Solar retinopathy: a multimodal analysis. Case Rep Ophthalmol Med. 2013;2013:906920.
- Venkatesh R, Pereira A, Singh V, Sangai S, Yadav NK. Multicolour imaging features in photic maculopathy. Clin Exp Optom. 2021 Mar;104(2):243-246.
- Das AV, Tyagi M, Kadam Y, Belenje A. Solar retinopathy in India: Clinical presentation and demographic distribution in 253 patients (349 eyes). Indian J Ophthalmol. 2023 May;71(5):2061-2065.
- Jain A, Desai RU, Charalel RA, Quiram P, Yannuzzi L, Sarraf D. Solar retinopathy: comparison of optical coherence tomography (OCT) and fluorescein angiography (FA). Retina. 2009 Oct; 29(9):p 1340-1345.
- Wu CY, Jansen ME, Andrade J, Chui TYP, Do AT, Rosen RB, Deobhakta A. Acute solar retinopathy imaged with adaptive optics, optical coherence tomography angiography, and en face optical coherence tomography. JAMA Ophthalmol. 2018 Jan 1;136(1):82-85.
- Yannuzzi LA, Fisher YL, Krueger A, Slakter J. Solar retinopathy: a photobiological and geophysical analysis. Trans Am Ophthalmol Soc. 1987;85:120-58.
- Abdellah MM, Mostafa EM, Anber MA, El Saman IS, Eldawla ME. Solar maculopathy: prognosis over one year follow up. BMC Ophthalmol. 2019 Sep 18;19(1):201.
- Augustin AJ. Zuverlässiger UV-Schutz durch Intraokularlinsen–Rationale und Qualitätsanforderungen [Reliable UV-light protection in intraocular lenses–scientific rationale and quality requirements]. Klin Monbl Augenheilkd. 2014 Sep;231(9):901-8. German. Epub 2014 Jul 3.
- Bouzas EA, Moret P, Pournaras CJ. Central serous chorioretinopathy complicating solar retinopathy treated with glucocorticoids. Graefes Arch Clin Exp Ophthalmol. 1999 Feb;237(2):166-8.
- Nakamura M, Komatsu K, Katagiri S, Hayashi T, Nakano T. Reconstruction of Photoreceptor Outer Layers after Steroid Therapy in Solar Retinopathy. Case Rep Ophthalmol Med. 2018 Jun 11;2018:7850467.
- Marashi A, Baba M, Zazo A. Managing solar retinopathy with suprachoroidal triamcinolone acetonide injection in a young girl: a case report. J Med Case Rep. 2021 Dec 2;15(1):577.
- Rai N, Thuladar L, Brandt F, Arden GB, Berninger TA. Solar retinopathy. A study from Nepal and from Germany. Doc Ophthalmol. 1998;95(2):99-108.

Dr. Rogers attended Illinois College of Optometry, and completed her residency there in Primary Care & Ocular Disease. She currently works at the VA in North Chicago.

{kind=link}