




Dolicoectatic Compression of the Optic Tract: A Case Report

 Save as PDF
Save as PDFABSTRACT
BACKGROUND
Dolichoectasia is an arterial disease that causes dilation or tortuosity of the impaired vessel. It most commonly affects the vertebrobasilar system and the internal carotid artery. Although most cases are asymptomatic, the condition may manifest by symptoms of headache, vertigo, visual disturbance, or signs of cranial nerve impairment. This case will discuss a patient being followed for low tension glaucoma who also had an undiagnosed intracranial dolichoectasia.
CASE REPORT
A 72-year-old male had been followed for low-tension glaucoma (LTG) for almost 10 years before uncovering a right hemianopsia. A neurological workup was conducted, revealing a dolichoectasia of the basilar artery causing compression of the left optic tract resulting in a visual field defect respecting the vertical midline. Although the initial diagnosis of LTG was confounded with the dolichoectasia, intraocular pressure lowering medication was continued as a precautionary measure.
CONCLUSION
This case highlights the importance of considering a possible underlying neurological etiology inpatients being followed for glaucoma. Visual fields are critical in helping to identify a neurological abnormality, paying close attention to symmetric defects that respect the vertical midline. These defects can be easily overlooked, especially if it occurs concomitantly with glaucoma. Abnormal neurological or visual findings can be life threatening and should be evaluated carefully to ensure they are not missed.
Keywords: dolichoectasia, vertebral basilar artery, normal tension glaucoma, hemianopsia
INTRODUCTION:
Dolichoectasia is a rare disorder of the cerebral vasculature that causes dilation and elongation of the impaired vessel. The vertebrobasilar system and internal carotid artery are most commonly affected.1,2 Vertebrobasilar dolichoectasia (VBD) is commonly associated with hypertension; however, congenital factors and other infectious causes have been identified.3,4 Although most cases are asymptomatic, headache, vertigo, and signs of cranial nerve impairment have been reported.7 As VBD progresses, compression on the neighboring neural structures can occur, which is the most common cause of the noted symptoms.5 Compression can also occur along the optic nerve pathway, causing visual field defects and disturbances. Some surgical treatment options are available depending on the location and extent of the dolichoectasia; however, these mostly aim to alleviate any compressive symptoms. No current therapies have been established to correct VBD specifically.3
CASE REPORT
A 72-year-old male was seen for an initial eye examination with a chief complaint of blurry vision. A complete eye exam was performed and with a small refractive error his best corrected visual acuity was 20/20 OD and 20/25 OS. The only noteworthy finding was a larger than average c/d ratio of 0.50V OD 0.40H OS with a deep cup description. He reported a head injury 12 years prior where he lost consciousness for 10 days with no apparent lasting effects. His medical history was significant for hypertension. A glaucoma workup was performed and showed open angles to the ciliary body OU with a flat iris approach and no pigment in the trabecular meshwork. His corneal pachymetry was slightly thin at 522 um OD and 525 um OS. His intraocular pressure (IOP) at this visit was 17mmHg OD and 19 mmHgOS but his maximum IOP eventually was documented to be 20 mmHg in each eye. Nerve fiber layer OCT findings (Figure 1a-b) were within normal limits for the right eye but showed thinning in the superior temporal quadrant of the left eye with corresponding inferior nasal defects with Humphrey visual field testing. The patient was subsequently diagnosed with low tension glaucoma (LTG) and treatment was initiated with Travatan. Over the next 9 years he was followed for glaucoma and exams demonstrated relative control of the condition, occasionally needing to change medication due to an allergic reaction or insufficient lowering of IOP when compared to target IOP of 13. The most recent topical medication he was prescribed was Simbrinza twice a day.

Figure 1a. Baseline RNFL OCT of the OD (left). Figure 1b. Baseline RNFL OCT of the OS (right)
During a routine follow-up exam 9 years following the initial diagnosis, the IOP was at 12mmHg OD and 13 mmHg OS. The c/d ratio remained unchanged based on fundoscopy, however, the RNFL on OCT demonstrated inferior temporal progression in the right eye and nasal progression in the left eye (Figures 1c and 1d). This was confirmed with ganglion cell analysis (Figures 2a and 2b).

Figure 1c and d. RNFL OCT of OD (left) and OS (right) 9 years from baseline.

Figure 2a (left): Ganglion cell layer showing thinning on the nasal portion. Figure 2b (right) Ganglion cell layer showing thinning on the temporal portion of the OS
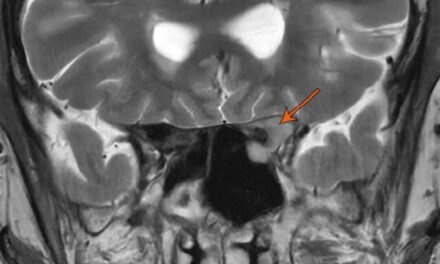
Visual field testing revealed a progressed visual field defect respecting the vertical midline consistent with a right hemianopsia (Figure 3). These visual field findings prompted obtaining MRI/MRA, which revealed dolichoectasia of the vertebrobasilar system with mass effect on the left optic tract at the level of the posterior cerebral artery (PCA) origins (Figure 4).

Figure 3. Humphrey Visual Fields showing emergence of right hemianopsia. TOP: Baseline. MIDDLE: 5 years from baseline. BOTTOM: 9 years from baseline.
Figure 4. MRI/MRA results revealed (left) dolichoectasia of the vertebrobasilar system with mass effect on the left optic tract at the level of the posterior cerebral artery (PCA) origins
After consulting with Neuro-ophthalmology and Neurosurgery specialties regarding the best treatment plan, it was determined that no viable intervention could be made for the dolichoectasia. Along with the blood pressure medication he was currently taking, 81 mg aspirin was prescribed. Additionally, it was difficult to distinguish whether the findings were solely due to the dolichoectasia or co-occurring with glaucoma, so IOP lowering treatment was continued. This decision was a conservative approach to avoid any vision loss from a preventable cause especially given the progressive nature of the defects that do correlate with the thinning on the OCT.
DISCUSSION
Dolichoectasia is an arterial disease that causes dilation or tortuosity of the impaired vessel. It is also referred to as dilatative arteriopathy because dilation seems to be the most important feature in its distinction.6 Intracranially, its prevalence is estimated to be around 5.8% of the general population and as high as 12% of those who have suffered a stroke.1,3 The overall survival rate was estimated to be between 36% and 60% in reported case series,8 with the 5-year prognosis being much better in patients who are asymptomatic at time of diagnosis.9
The clinical manifestations of VBD can be separated into compressive symptoms and vascular events. Compressive symptoms create a mass effect on the surrounding cranial nerves and neural structures, while vascular events manifest as TIA’s, hemorrhage, dissection, or stroke.4,10 One way these vascular events occur was demonstrated through transcranial doppler studies showing reduced blood flow in dolichoectatic arteries causing stagnation and reduced antegrade flow. This increases the risk of intracranial ischemia through thrombus formation, atherosclerotic plaques, and fibrotic changes in the vessel wall.8,11 The most common symptom from a vascular event is ischemic stroke, which is also the most common cause of death related to VBD.12
Although most cases of VBD are asymptomatic; headache, vertigo, and signs of cranial nerve impairment are reported as most common.7 The most common cause of these symptoms is from compression on the neighboring neural structures as VBD progresses.5 This compression can also occur along the optic nerve pathway, causing visual field defects and disturbances. It is, however, rarely noted in the literature for a post chiasmal compression from VBD to cause a hemianopsia as in the presented case. A literature review conducted in 2018 found that only 6 cases fell into this category, while the majority occurred from internal carotid compression.13 Most frequently, hemianopsias are caused by cerebral infarcts and intracranial hemorrhages (42%-89%), while other causes are from tumors, trauma, iatrogenic, and neurological disease.14
Several studies have shown a connection between arterial hypertension and the formation of intracranial dolichoectasia, as well as being a contributing factor in stroke and intracranial hemorrhage.15,16 Consequently, arterial blood pressure control is believed to be the best management strategy for dolichoectasia.17 Anti-coagulant or platelet therapy has also been recommended as a possible treatment option, although this is controversial due to some studies showing an increase in intracranial bleeding. Others reason that the increased risk of bleeding is outweighed by the possibility of stroke in patients with VBD not on anticoagulant therapy. 9,17,18 In this case, aspirin was prescribed to the patient for this reason. Interestingly, one study found that the lack of prior anticoagulant use was an independent predictor of all-cause mortality compared to controls.9 Smoking has also been noted to be a modifiable risk factor and may assist in convincing a patient to quit who also has intracranial dolichoectasia.18 Depending on the extent and location of the dolichoectasia, surgical options are available but are performed mostly to relieve the compressive symptoms. This includes parent vessel occlusion, clip reconstruction, and transposition or wrapping of the affected vessel.3,17 Currently however, there is no established treatment to correct VBD.
Glaucoma usually affects the nasal or superior visual field in early glaucoma, sometimes respecting the horizontal midline.19 If any visual field respects the vertical midline, further evaluation must take place as this may be indicative of a neurological issue. In the case discussed, two findings did not match the typical disease progression. First, one would expect more inferior RNFL thinning of the left eye to correlate with the visual field progression into the superior quadrant. Secondly, a right hemianopsia was uncovered, pointing to disruption of the visual pathways within the central nervous system and not glaucoma.20
It is important to note that these defects need not be dense in order to detect an abnormality. Figure 3 shows that the right eye defects are not as severe as the left with only a few points showing symmetry, however this is enough to warrant neuroimaging. The defects can fluctuate with the variability of the visual field along with the symptoms experienced by those who suffer from the dolichoectasia. One paper highlights such a case where symptoms fluctuate depending on head position, due to how gravity affected the intracranial vessel position and its mass effect on neighboring structures.21
Any infarction or insult along the visual pathway can cause retrograde degeneration of retinal ganglion cells. This can be detected through degeneration of the macular ganglion cell layer (GCL) on OCT. 22 Figures 2a and 2b show GCL thinning nasally in the right eye and temporally in the left eye, correlating with the noted right hemianopsia (Figure 3). This further supports the relationship between the mass effect from the dolichoectatic vessel on the optic nerve and the visual field defect.
Clinically, there are no indicators that would point to a dolichoectatic vessel over another cause of optic nerve pathology on presentation of a neurological visual field. Interestingly, the presented case follows the most common way that intracranial dolichoectasia is discovered, which is when patients being followed for low-tension glaucoma are later found to have vascular compression of neural structures when atypical progression is noted.23 Gutman et al found that of 62 patients with classic LTG signs, 56 of them showed displacement of the optic nerve by carotid compression.24 Of these, 28 (45.2%) patients showed optic nerve cupping asymmetry which correlated with the severity of the carotid artery pathology.24 This supports a causal relationship between optic nerve findings and mass effect from the abnormal vessels, which may occur more often than previously believed.
CONCLUSION:
Clinicians must be cognizant of a possible underlying neurological etiology or co-occurring disease with any glaucoma patient, especially in normotensive glaucoma. This may not be apparent on initial diagnosis but should always be considered as more data is acquired or when progression is atypical for glaucoma. Visual fields are critical in helping to reveal a neurological abnormality, specifically defects that respect the vertical midline or that are symmetrical in nature.
REFERENCES:
- Kawahara I, Morofuji Y, Takahata H, Toda K, Tsutsumi K, Baba H, Yonekura M. Dolichoectasic anterior cerebral artery and hemodynamics. J Stroke Cerebrovasc Dis. 2012 Nov;21(8):907.e5-8. doi: 10.1016/j.jstrokecerebrovasdis.2011.07.017. Epub 2011 Oct 6. PMID: 21982268.
- Yu YL, Moseley IF, Pullicino P, McDonald WI. The clinical picture of ectasia of the intracerebral arteries. J Neurol Neurosurg Psychiatry. 1982 Jan;45(1):29-36. doi: 10.1136/jnnp.45.1.29. PMID: 7062068; PMCID: PMC491261.
- Gutierrez, J., Sacco, R. & Wright, C. Dolichoectasia—an evolving arterial disease. Nat Rev Neurol7, 41–50 (2011). https://doi.org/10.1038/nrneurol.2010.181
- Yuan YJ, Xu K, Luo Q, Yu JL. Research progress on vertebrobasilar dolichoectasia. Int J Med Sci. 2014 Aug 2;11(10):1039-48. doi: 10.7150/ijms.8566. PMID: 25136259; PMCID: PMC4135226
- Uchino A, Kohyama S. Long segment dolichoectasia of the right internal carotid artery diagnosed by CT angiography. Radiol Case Rep. 2019 Jul 10;14(9):1084-1087. doi: 10.1016/j.radcr.2019.06.013. PMID: 31338131; PMCID: PMC6625973.
- Caplan LR. Dilatative arteriopathy (dolichoectasia): What is known and not known. Ann Neurol. 2005 Apr;57(4):469-71. doi: 10.1002/ana.20447. PMID: 15786452.
- Baran B, Kornafel O, Guziński M, Sąsiadek M. Dolichoectasia of the circle of Willis arteries and fusiform aneurysm of basilar artery – case report and review of the literature. Pol J Radiol. 2012 Apr;77(2):54-9. doi: 10.12659/pjr.882971. PMID: 22844310; PMCID: PMC3403802
- Milandre L, Bonnefoi B, Pestre P, Pellissier JF, Grisoli F, Khalil R. Dolichoectasies artérielles vertébrobasilaires. Complications et pronostic [Vertebrobasilar arterial dolichoectasia. Complications and prognosis]. Rev Neurol (Paris). 1991;147(11):714-22. French. PMID: 1775825.
- Wolters F, Rinkel G, Vergouwen M. Clinical Course and Treatment of Vertebrobasilar Dolichoectasia: A Systematic Review of the Literature. Neurological Research. 2013;35(2):131-7. doi:10.1179/1743132812y.0000000149
- Holmes BB, Green WC, Kung NH, Goebel JA, Van Stavern GP. Vertebrobasilar Dolichoectasia Causing An Optic Tract Syndrome. J Neuroophthalmol. 2017 Jun;37(2):179-181. doi: 10.1097/WNO.0000000000000495. PMID: 28350571.
- Hennerici M, Rautenberg W, Sitzer G, Schwartz A. Transcranial Doppler ultrasound for the assessment of intracranial arterial flow velocity–Part 1. Examination technique and normal values. Surg Neurol. 1987 May;27(5):439-48. doi: 10.1016/0090-3019(87)90251-5. PMID: 2951884.
- Del Brutto VJ, Ortiz JG, Biller J. Intracranial Arterial Dolichoectasia. Front Neurol. 2017 Jul 17;8:344. doi: 10.3389/fneur.2017.00344. PMID: 28769872; PMCID: PMC5511833.
- Greuter L, Fournier JY. Vertebrobasilar dolichoectasia causing homonymous hemianopia: a case report and review of the literature. Acta Neurochir (Wien). 2018 Jan;160(1):161-164. doi: 10.1007/s00701-017-3367-x. Epub 2017 Oct 26. PMID: 29075905.
- Wolberg A, Kapoor N. Homonymous Hemianopsia. [Updated 2022 Jun 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK558929/
- Dandapani BK, Suzuki S, Kelley RE, Reyes-Iglesias Y, Duncan RC. Relation between blood pressure and outcome in intracerebral hemorrhage. Stroke. 1995 Jan;26(1):21-4. doi: 10.1161/01.str.26.1.21. PMID: 7839391.
- Dickinson CJ. Strokes and their relationship to hypertension. Curr Opin Nephrol Hypertens. 2003 Jan;12(1):91-6. doi: 10.1097/00041552-200301000-00015. PMID: 12496672.
- Lin YW, Chen CH, Lai ML. The dilemma of treating vertebrobasilar dolichoectasia. Clin Pract. 2012 Oct 17;2(4):e84. doi: 10.4081/cp.2012.e84. PMID: 24765483; PMCID: PMC3981198.
- Wolfe T, Ubogu EE, Fernandes-Filho JA, Zaidat OO. Predictors of clinical outcome and mortality in vertebrobasilar dolichoectasia diagnosed by magnetic resonance angiography. J Stroke Cerebrovasc Dis. 2008 Nov-Dec;17(6):388-93. doi: 10.1016/j.jstrokecerebrovasdis.2008.06.006. PMID: 18984433.
- Phelps CD, Hayreh SS, Montague PR. Comparison of visual field defects in the low-tension glaucomas with those in the high-tension glaucomas. Am J Ophthalmol. 1984 Dec 15;98(6):823-5. doi: 10.1016/0002-9394(84)90721-9. PMID: 6507569.
- Ruddy J, Cardenas AC. Hemianopsia. 2023 May 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 32965933.
- Payton Yerke Hansen, Katelyn L. Seeley, Duane L. Tanner. Optic Nerve Compression due to Dolichoectasia: a Teaching Case Report [Internet]. 2023 winter-spring[cited Jan2024] [about 4 pages]Vol48(2). Optic Nerve Compression due to Dolichoectasia:a Teaching Case Report | The Journal of Optometric Education (opted.org)
- Herro AM, Lam BL. Retrograde degeneration of retinal ganglion cells in homonymous hemianopsia. Clin Ophthalmol. 2015 Jun 11;9:1057-64. doi: 10.2147/OPTH.S81749. PMID: 26089638; PMCID: PMC4468984.
- Elmalem VI, Purvin VA. Does Dolichoectasia of the Carotid Artery Cause Optic Neuropathy? J Neuroophthalmol. 2018 Sep;38(3):368-374. doi: 10.1097/WNO.0000000000000653. PMID: 29613917.
- Gutman I, Melamed S, Ashkenazi I, Blumenthal M. Optic nerve compression by carotid arteries in low-tension glaucoma. Graefes Arch Clin Exp Ophthalmol. 1993 Dec;231(12):711-7. doi: 10.1007/BF00919286. PMID: 8299979.

Dr. Terry is an attending optometrist at the Salt Lake City VA Medical Center where he completed his Primary Care/Contact lens residency in 2017 and currently directs the specialty contact lens clinic. He is adjunct assistant professor at several optometry schools and maintains ABCMO certification.


{kind=link}