




Recurrent Conjunctival Squamous Papilloma

 Save as PDF
Save as PDFABSTRACT
BACKGROUND
Nonmelanocytic conjunctival tumors of the epithelium are slightly elevated, variably shaped, sharply demarcated from surrounding normal tissues, and range in color from pearly gray to reddish depending on vascularity.1,2 These tumors can range from benign lesions such as a conjunctival squamous papilloma to malignant squamous cell carcinoma (SCC).3,4,5 With similarity in appearance amongst nonmelanocytic conjunctival tumors, biopsy is essential to differentiate these lesions.1,2,6 Treatments such as cryotherapy or other topical therapies can be used in conjunction with surgical removal to decrease recurrence.1,2,6,7
CASE REPORT
This case features a 76-year-old Caucasian male with a conjunctival squamous papilloma regrowth. The initial lesion was removed solely via excisional biopsy, and the recurrent lesion was treated via excisional biopsy with adjunctive cryotherapy.
CONCLUSION
This report reviews different epithelial conjunctival tumors and their necessary treatment and management considerations.
Keywords: conjunctival tumors, conjunctival squamous papilloma, conjunctival intraepithelial neoplasia, squamous cell carcinoma
INTRODUCTION
Conjunctival tumors include a wide spectrum of neoplasms ranging from benign squamous papilloma to conjunctival intraepithelial neoplasia (CIN) and malignant squamous cell carcinoma (SCC).3,4,5 Although the incidence of conjunctival tumors is rare, the rate of malignancy is 30%.5 Conjunctival tumors most commonly affect Caucasians and present in middle-aged individuals.3 Predisposing factors include ultraviolet-B exposure (UV-B) and human papillomavirus (HPV) infection.1,2,5 Biopsy is essential in the diagnosis of conjunctival tumors because benign and malignant lesions have similar features. Recurrence of conjunctival tumors is as high as 41% in SCC.1 Cryotherapy and topical treatments have been found to be effective supplemental treatments following excision of conjunctival tumors.6
CASE PRESENTATION
A 76-year-old male presented to the clinic for a right bulbar conjunctival lesion. During ocular history, the patient reported a similar lesion had been excised two years prior by another provider. Exact onset of the regrowth was unclear, although the patient reported that the lesion began interfering with blinking two months prior. The patient denied changes in vision, headaches, dizziness, diplopia, and eye pain.
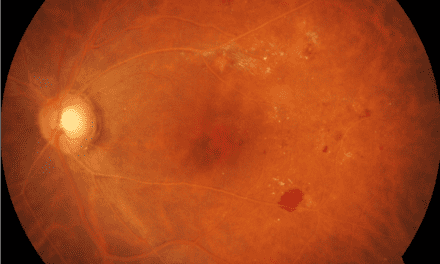
Previous record review showed the initial conjunctival lesion was removed via shave biopsy, and the pathology report confirmed a squamous papilloma. An anterior segment photo of the lesion prior to excision was included (Figure 1).

Figure 1. Conjunctival lesion of right eye prior to the first excision (two years prior)
The patient’s medical history included essential hypertension, chronic kidney disease, hyperlipidemia, diabetes mellitus type 2, cerebrovascular disease, and recent SCC. The SCC was located on the patient’s left ear and was removed with Mohs surgery. The patient’s medications included metoprolol, atorvastatin, losartan, metformin, and aspirin.
Best-corrected visual acuities were 20/20 in each eye and entrance tests were unremarkable. Anterior segment evaluation revealed clear lids and lashes OD and OS, clear and intact cornea OD and OS, a sessile, gelatinous, immobile, vascularized lesion that measured 4 mm x 3.5 mm on the inferior bulbar conjunctiva without corneal involvement OD (Figure 2), white and quiet bulbar conjunctiva OS, clear and quiet palpebral conjunctiva OD and OS, deep and quiet anterior chamber OD and OS, and flat irides without neovascularization OD and OS. IOP measured 9 mmHg OD and 9 mmHg OS with Goldmann applanation tonometry. Posterior segment evaluation revealed incipient cataracts OD and OS and was otherwise unremarkable.

Figure 2. Recurrent conjunctival lesion of right eye prior to the second excision
DIFFERENTIAL DIAGNOSES
Squamous papilloma of the conjunctiva appears as a gelatinous, pedunculated or sessile, red or pink fibrovascular frond lesion.6,8 Squamous papillomas are benign lesions which can be located on the bulbar or palpebral conjunctiva.9 In children, papillomas are most commonly located in the inferior fornix, whereas in adults, papillomas are often located near the limbus and extend onto the cornea.6,9 A conjunctival squamous papilloma was the leading differential for this patient due to the appearance of the lesion, as well as the previously confirmed diagnosis of squamous papilloma.
CIN appears as a minimally elevated, gelatinous, white or grey-white, sessile lesion.6,9,10 CIN can also present with a papillomatous, fern-like appearance.9 A white plaque can develop on the surface of the lesion secondary to hyperkeratosis.6 These lesions are premalignant and can lead to development of SCC. CIN most commonly begins at the limbus in the interpalpebral fissure and can extend onto the adjacent cornea.6,9 CIN less commonly occurs in the forniceal or palpebral conjunctiva.6
Conjunctival SCC has a gelatinous, exophytic, papillary appearance with loops of abnormal blood vessels.10 Conjunctival SCC is typically located in the interpalpebral region with potential extension onto the adjacent cornea.10 Conjunctival SCC is characterized by malignant squamous cells that breach the basement membrane and grow into the adjacent stromal tissue.6
Due to the similar clinical presentation of these differentials, regrowth, and patient’s systemic history, a biopsy was necessary for definitive diagnosis.
BIOPSY RESULTS
Excision biopsy of the inferior conjunctiva with underlying sclera with double thaw cryotherapy of the inferior conjunctiva was simultaneously performed in another clinic. The biopsy results confirmed the diagnosis of a benign squamous papilloma.
DISCUSSION
The incidence of conjunctival tumors has been found to be between 0.13/100,000 and 1.9/100,000.1,2 Conjunctival tumors present at a mean age of 50 years, have no predilection for sex (51% males vs 49% females), and have a higher prevalence in Caucasians (83%).3 Geographic distribution of those who live within 30 degrees latitude of the equator impacts the prevalence of conjunctival tumor development in younger and darker skinned populations.2 Conjunctival tumors are also more apt to occur in those exposed to years of solar radiation through activities such as golfing, fishing, boating, construction, and farming.5 Both increased UV-B exposure from geography or lifestyle and human papillomavirus have been found to disrupt limbal stem cells which are responsible for corneal epithelial replacement. When the regulatory mechanism of these limbal stem cells is altered, the abnormal epithelial phenotypes, accompanied by neovascularization, alter the basement membrane, causing infiltration of inflammatory cells and creation of conjunctival lesions. 1
The spectrum of conjunctival tumors is wide, but conjunctival lesions can be further broken down into categories based on severity, age of onset, and cell types in which the tumor originates.3,5,6 Based on severity, conjunctival tumors are classified as benign (52%), premalignant (18%), or malignant (30%).5 Based on age of onset, conjunctival tumors can be identified by congenital versus acquired. Lastly, classifications can be based on the cells in which the tumor originates: melanocytic (53%) or nonmelanocytic (47%).3
Nonmelanocytic conjunctival tumors of the epithelium, as seen this case, are most commonly described as slightly elevated, variably shaped, sharply demarcated from surrounding normal tissues, and ranging in color from pearly gray to reddish depending on vascularity of the tumor.1,2 Clinical presentation can be described as gelatinous, papilliform or velvety, or leukoplakic, with gelatinous lesions the most common appearance.1 Nonmelanocytic conjunctival tumors are most commonly located at the limbus (74%), but can also be found solely on the conjunctiva.1,2,3 The lesion typically presents in the interpalpebral fissure, as this is the most sun exposed region.5
Histopathology of nonmelanocytic conjunctival tumors reveals epithelial dysplasia.1,2 The presence of epithelial disarray and abnormalities in maturation is the pathologic basis for a lesion to be classified as preinvasive.2 An abrupt demarcation line is generally found at the edges of a preinvasive conjunctival tumor.2 The severity of a preinvasive lesion is classified according to the degree of dysplastic epithelial involvement, with severe lesions demonstrating dysplasia that extends into the upper third of the epithelium.2 Conjunctival lesions are considered invasive and malignant when a nest of infiltrating cells has penetrated the basement membrane of the epithelium and invaded the conjunctival stroma.1,2
In addition to invasion of surrounding ocular tissues as mentioned above, malignant conjunctival tumors provide concern for systemic involvement. The risk of premalignant and malignant conjunctival epithelial lesions metastasizing to regional lymph nodes is less than 10%, and the risk to distant sites is rare.11 However, for conjunctival melanomas, the risk of metastasis to distant sites is 10-30%.11 According to Shields et al, 32% of patients with conjunctival melanomas develop metastasis by 15 years with ipsilateral facial lymph nodes, brain, lung, and liver being the most common sites of metastasis.6
Due to easy visualization of the conjunctiva by patients and providers, conjunctival tumors are generally identified in the early stages.6 It is essential to evaluate the cornea in cases of conjunctival tumors, as invasion of the peripheral cornea can be seen as a subtle, gray opacity.6 Rose Bengal has been found to be a useful tool to help delineate the tumors.4 Another useful tool in the evaluation of conjunctival tumors is an anterior segment optical coherence tomography (AS-OCT).7 AS-OCT has shown severely thickened, hyperreflective epithelium with an abrupt transition between the normal and affected epithelium as compared to benign lesions.12 This minimally invasive technology was found to be a great tool for monitoring conjunctival lesions, and also helped provide a diagnosis of conjunctival tumors based on epithelial thickness.12
Biopsy to confirm the diagnosis of the conjunctival tumor is most appropriate for management recommendations. For tumors that are benign and asymptomatic, observation is sufficient.6 The provider should look for evidence of growth, malignant change, or secondary effects on normal tissues at follow-up visits.6
Excision of the lesion allows for rapid resolution. Despite this, subclinical microscopic diseases beyond the region of excision can remain, thus causing recurrences.6 For this reason, chemotherapeutic options have been studied. Research has found that epithelial malignancies can be treated with topical medications that contain mitomycin C (MMC), 5-Fluorouracil (5FU), or interferon (interferon alpha-2b).1,2,6,7,8 These topical treatments are most effective with lesions that are intraepithelial versus lesions affecting deeper tissues.6 MMC is an alkylating agent that acts in all phases of the cell cycle and inhibits RNA and protein synthesis.7 5FU is an antimetabolite that inhibits the action of thymidylate synthase therefore interrupting the synthesis of nucleosides used for DNA formation.7 Interferon is an endogenous glycoprotein released by various immune cells with antiviral, antimicrobial, and antineoplastic activities.7 Because of the ocular toxicity of these medications, the medications are given and then followed by an off period to allow recovery of the ocular tissue.6,7 Variation in recurrence rates following these different topical medications also exists.7 After 5FU, 11.5% recurrence was noted, whereas 5.1% recurrence after IFN was noted.7
Cryotherapy is also used as an additional treatment option when performing an excisional biopsy.6 Cryotherapy destroys cells via thermal effect while obliterating the microcirculation causing ischemic infarction of the area.2 It effectively disrupts superficial tumor islands and deeply infiltrated tumor cells.2 Cryotherapy is advantageous to perform while doing an excisional biopsy because it eliminates subclinical tumor cells that are unable to be removed during excisional biopsy as well as reduces recurrence.1,6
Recurrence rates for preinvasive and invasive conjunctival tumors vary and depend mostly on surgical margins rather than any particular patient characteristic or clinical appearance of the lesion.1 Recurrence rates for preinvasive and invasive conjunctival tumors following surgical excisions range from 5% when pathology reports confirmed clear margins to 53% when pathology showed involved margins.2 Other than surgical margins, severity also plays a minor role in recurrence with there being a higher rate of recurrence with more severe grades of conjunctival tumors, such as premalignant and malignant conjunctival tumors.1 This was noted between CIN and SCC with a 24% recurrence in CIN and 41% recurrence in SCC.1 Conjunctival tumor recurrence was most likely to occur within two years following removal of the initial lesion.2 Second recurrence is also likely, with a 31% chance of second recurrence occurring between three months and five years following removal of the initial lesion.1
Recurrences of conjunctival tumors vary depending on the type of conjunctival tumor and the type of treatment. In conjunctival squamous papillomas, average recurrence rate has been found to be up to 22.5% and reoccur in up to 25% of cases.8,13,14 Recurrences vary greatly however, depending on whether or not adjunctive therapy was performed.14 A study by Huang et al found 50% recurrence with excision only compared to 7.1% recurrence with adjunctive therapy: cryotherapy and/or topical MMC.14
CONCLUSION
The different types of nonmelanocytic conjunctival tumors of the epithelium share many clinical features.1,2,6 Although systemic malignancy of all conjunctival tumors is infrequent, prompt diagnosis and proper management is essential to prevent invasion of surrounding ocular tissue.2,6,10,11 This case demonstrates the importance of patient history, clinical observation, and referral to obtain biopsy for accurate diagnosis and tailored management recommendation for patients with suspicious conjunctival lesions. When suspicious for malignancy, biopsy is essential to make the correct diagnosis.1,2,6 Adjunctive therapies such as cryotherapy and/or topical therapies are advantageous as they decrease the risk of recurrences by removing the subclinical tumor cells.1,2,6,7,8 With early detection, diagnosis, and treatment, prognosis for individuals with conjunctival tumors is favorable.6
REFERENCES
- Lee, G. A., & Hirst, L. W. (1995). Ocular surface squamous neoplasia. Survey of ophthalmology, 39(6), 429–450. https://doi.org/10.1016/s0039-6257(05)80054-2
- Basti, S., & Macsai, M. S. (2003). Ocular surface squamous neoplasia: a review. Cornea, 22(7), 687–704. https://doi.org/10.1097/00003226-200310000-00015
- Shields, C. L., Alset, A. E., Boal, N. S., Casey, M. G., Knapp, A. N., & Sugarman, M. A. (2017). Conjunctival Tumors in 5002 Cases. Comparative Analysis of Benign Versus Malignant Counterparts. The 2016 James D. Malignant Counterparts. The 2016 James D. Allen Lecture. American Journal of Ophthalmology. 173, 106-133. https://doi.org/10.1016/j.ajo.2016.09.034
- Honavar, S. G., & Manjandavida, F. P. (2015). Tumors of the ocular surface: A review. Indian journal of ophthalmology, 63(3), 187–203. https://doi.org/10.4103/0301-4738.156912
- Shields, C. L., Chien, J. L., Surakiatchanukul, T., Sioufi, K., Lally, S. E., & Shields, J. A. (2017). Conjunctival Tumors: Review of Clinical Features, Risks, Biomarkers, and Outcomes-The 2017 J. Donald M. Gass Lecture. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.), 6(2), 109–120. https://doi.org/10.22608/APO.201710
- Shields, C. L., & Shields, J. A. (2004). Tumors of the conjunctiva and cornea. Survey of ophthalmology, 49(1), 3–24. https://doi.org/10.1016/j.survophthal.2003.10.008
- Venkateswaran, N., Mercado, C., Galor, A., & Karp, C. L. (2019). Comparison of Topical 5-Fluorouracil and Interferon Alfa-2b as Primary Treatment Modalities for Ocular Surface Squamous Neoplasia. American journal of ophthalmology, 199, 216–222. https://doi.org/10.1016/j.ajo.2018.11.007
- Kanski, J. J. (2007). Conjunctiva. In Clinical Ophthalmology: A Systemic Approach. Oxford: Butterworth Heinemann Elsevier.
- Bagheri, N. (2017). Conjunctiva/Sclera/Iris/External Disease. In The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. Philadelphia: Wolters Kluwer.
- Friedman, N. J., Kaiser, P. K., & Pineda, R. (2009). Conjunctiva and Sclera. In The Massachusetts Eye and Ear Infirmary illustrated manual of ophthalmology. St. Louis, MO: Elsevier.
- Kaan Gündüz & Bita Esmaeli (2008) Diagnosis and management of malignant tumors of the eyelid, conjunctiva and orbit, Expert Review of Ophthalmology, 3:1, 63-75, DOI: 10.1586/17469899.3.1.63
- Kieval, J. Z., Karp, C. L., Abou Shousha, M., Galor, A., Hoffman, R. A., Dubovy, S. R., & Wang, J. (2012). Ultra-high resolution optical coherence tomography for differentiation of ocular surface squamous neoplasia and pterygia. Ophthalmology, 119(3), 481–486. https://doi.org/10.1016/j.ophtha.2011.08.028
- Hanbazazh, M., & Gyure, K. A. (2018). Ocular Human Papillomavirus Infections. Arch Pathol Lab Med, 12(6), 706–710. https://doi.org/10.5858/arpa.2017-0571-RA
- Huang, Y. M., Huang, Y. Y., Yang, H. Y., Tsai, C. C., Yu, W. K., Kao, S. C., Kau, H. C., & Liu, C. J. (2018). Conjunctival papilloma: Clinical features, outcome, and factors related to recurrence. Taiwan journal of ophthalmology, 8(1), 15–18. https://doi.org/10.4103/tjo.tjo_2_18

Dr. Wittendorf is a 2020 graduate of the Michigan College of Optometry. Upon graduation, she completed an ocular disease residency with the Battle Creek VAMC. She currently practices at the Jackie Walorski VA serving as the student externship director.

Dr. Gilbertson Kuiken is an attending optometrist at the Battle Creek Veterans Affairs Medical Center where she completed her ocular disease residency in 2012. She is a Fellow of the American Academy of Optometry and maintains ABCMO certification.

Dr. Vanderpool is a Fellow of the American Academy of Optometry and Certified in the Specialty of Medical Optometry (ABCMO). She completed her residency in ocular disease at the Battle Creek Veterans Affairs Medical Center, where she has been an attending optometrist for the past 7 years.



{kind=link}